CHI Health Creighton University Medical Center Omaha, NE
Aditya Avula, DO, Shalini S. Jain, MD CHI Health Creighton University Medical Center, Omaha, NE Introduction: Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin’s lymphoma, accounting for approximately 30%-40% of cases. DLBCL typically presents in lymph nodes, however the gastrointestinal (GI) tract is one of the most common extra-nodal sites. The stomach is the most affected GI site, while duodenal involvement is particularly rare.
Case Description/
Methods: An immunocompetent 69-year-old male with history of chronic burning epigastric pain and recent 100-pound weight loss presented after a syncopal event. He had previous work up for his symptoms including Esophagogastroduodenoscopy (EGD) with Endoscopic Ultrasound (EUS), which revealed chronic gastritis and increased lymphoid aggregates seen in the duodenal mucosa. Laboratory evaluation was unremarkable except for fecal calprotectin (FCP) elevated at 1530 ug/ml. Trials of omeprazole and sucralfate did not improve his symptoms.
In the emergency department, evaluation with CT abdomen/pelvis revealed a 3.8 cm mass thought to be in the gastric fundus. EGD revealed a polypoid lesion without bleeding in the first portion of the duodenum. There was localized severe mucosal changes characterized by thickening, erythema, and prolapsing in the apex of the duodenal bulb. EUS showed diffuse wall thickening measuring 11.4 mm within the luminal superficial mucosa, deep mucosa, and submucosa. Biopsies were taken with cold forceps, which revealed diffuse large B-cell lymphoma, non-germinal center type. Gastric biopsies showed evidence of chronic gastritis negative for Helicobacter pylori infection. Fluorescence in situ hybridization (FISH) analysis was negative for any genetic abnormalities. The patient was referred to oncology for further evaluation and treatment. Discussion: Risk factors for GI lymphomas include immunosuppressive states, viral infection, and autoimmune conditions. They are commonly found in the second part of the duodenum and can often initially be misinterpreted as Brunner’s gland hyperplasia. Majority of patients are incidentally found on endoscopy. This patient was also found to have elevated FCP two years prior, which has been shown to be diagnostic for gastric lymphomas. Although surveillance is often the first approach to determining if further aggressive treatment, such as chemotherapy, is warranted, risk for transformation to high grade lymphoma can occur in about 23%. Therefore, this case highlights the importance of keeping DLBCL in the differential as a rare cause of GI malignancy.
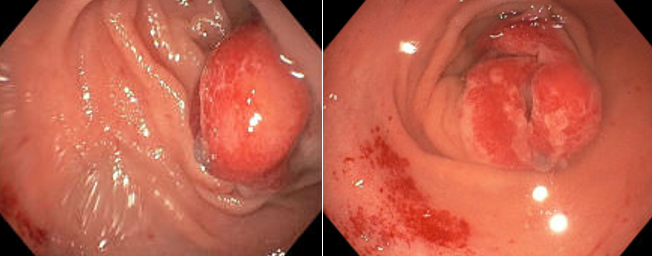
Figure: Polypoid lesion in the first portion of the duodenum with localized severe mucosal changes characterized by thickening, erythema, and prolapsing in the apex of the duodenal bulb.
Figure: Endoscopic ultrasound image depicting wall thickening at the apex of the duodenal bulb within the luminal superficial mucosa, deep mucosa, and submucosal layers
Disclosures: Aditya Avula indicated no relevant financial relationships. Shalini Jain indicated no relevant financial relationships.
Aditya Avula, DO, Shalini S. Jain, MD. P1969 - A Case of Duodenal Diffuse Large B-cell Lymphoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.