Urmimala Chaudhuri, DO1, Yesol Oh, MD2, Rawan Aljaras, MD3, Drew Triplett, DO3 1Wright State University, Centerville, OH; 2Wright State University, Dayton, OH; 3Wright State University Boonshoft School of Medicine, Dayton, OH Introduction: Duodenal follicular lymphoma (DFL) is a rare variant of non-Hodgkin’s lymphoma typically localized to the second part of the duodenum. It typically presents without symptoms and is associated with a favorable prognosis. Here, we discuss two cases of primary DFL with differing clinical presentations, emphasizing the role of endoscopic diagnosis and individualized management strategies.
Case Description/
Methods: Case 1:
A 60-year-old female was evaluated at the gastroenterology clinic for symptoms of rectal bleeding, abdominal bloating, cramping, and dysphagia. Esophagogastroduodenoscopy (EGD) revealed retained fibrous food in the stomach, gastritis, and a duodenal polyp. Duodenal biopsies for the polyp demonstrated dense lymphoid infiltrates consistent with follicular lymphoma. Positron emission tomography/computed tomography (PET/CT) and bone marrow biopsy showed no evidence of systemic involvement, confirming the diagnosis of primary DFL. The patient was counseled on treatment options including active surveillance, radiation therapy, or rituximab monotherapy. Given the indolent nature of DFL and absence of systemic disease, she opted for active surveillance.
Case 2:
A 70-year-old female was evaluated following hospitalization for small bowel obstruction (SBO). EGD revealed 20 mm duodenal polyp, and biopsy confirmed low-grade follicular lymphoma. As with the first case, staging studies did not show systemic involvement of the disease. Due to the lesion’s size and recent SBO, radiation therapy was recommended. Discussion: Primary DFL can be detected incidentally during endoscopy for unrelated symptoms. Characteristic endoscopic findings include whitish, polypoid, or nodular lesions in the second portion of the duodenum. Diagnosis is confirmed with histopathology and immunohistochemistry. DFL generally follows an indolent course but has a favorable prognosis.
Management is guided by disease burden and clinical presentation. In asymptomatic patients with no systemic disease, a watchful waiting strategy is appropriate, with studies reporting disease stability or spontaneous regression in up to 70% of cases. In contrast, patients with complications such as SBO or large unresected lesions may require definitive therapy, including radiation, to prevent local progression or recurrence. These cases emphasize the importance of recognizing DFL during endoscopy, and tailoring treatment based on individual risk and extent of the disease.
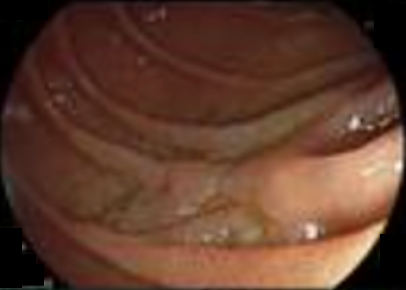
Figure: Figure 1. EGD findings from Case 1. 60-year-old female found to have 15 mm polyp in the second part of the duodenum which was confirmed to be duodenal follicular lymphoma on biopsy.
Figure: Figure 2. EGD findings from Case 2. 70 year-old female found to have 20 mm polyp in the second part of the duodenum which was confirmed to be duodenal follicular lymphoma on biopsy.
Disclosures: Urmimala Chaudhuri indicated no relevant financial relationships. Yesol Oh indicated no relevant financial relationships. Rawan Aljaras indicated no relevant financial relationships. Drew Triplett indicated no relevant financial relationships.
Urmimala Chaudhuri, DO1, Yesol Oh, MD2, Rawan Aljaras, MD3, Drew Triplett, DO3. P1966 - Duodenal Follicular Lymphoma: A Case Series of Endoscopic Recognition and Risk-Stratified Management, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.