Penn State Health Milton S. Hershey Medical Center Hershey, PA
Karen Krok, MD, Smriti Kochhar, DO, Mikayla Cochrane, MD, BS Penn State Health Milton S. Hershey Medical Center, Hershey, PA Introduction: Granulomatous hepatitis (GH) refers to the presence of granulomas, organized collections of macrophages, with multinucleated giant cells, within the liver parenchyma. It is a histopathological finding rather than a specific disease entity and can be associated with a broad range of etiologies, including infectious, autoimmune, drug-induced, neoplastic, and idiopathic causes. Management is etiology specific.
Case Description/
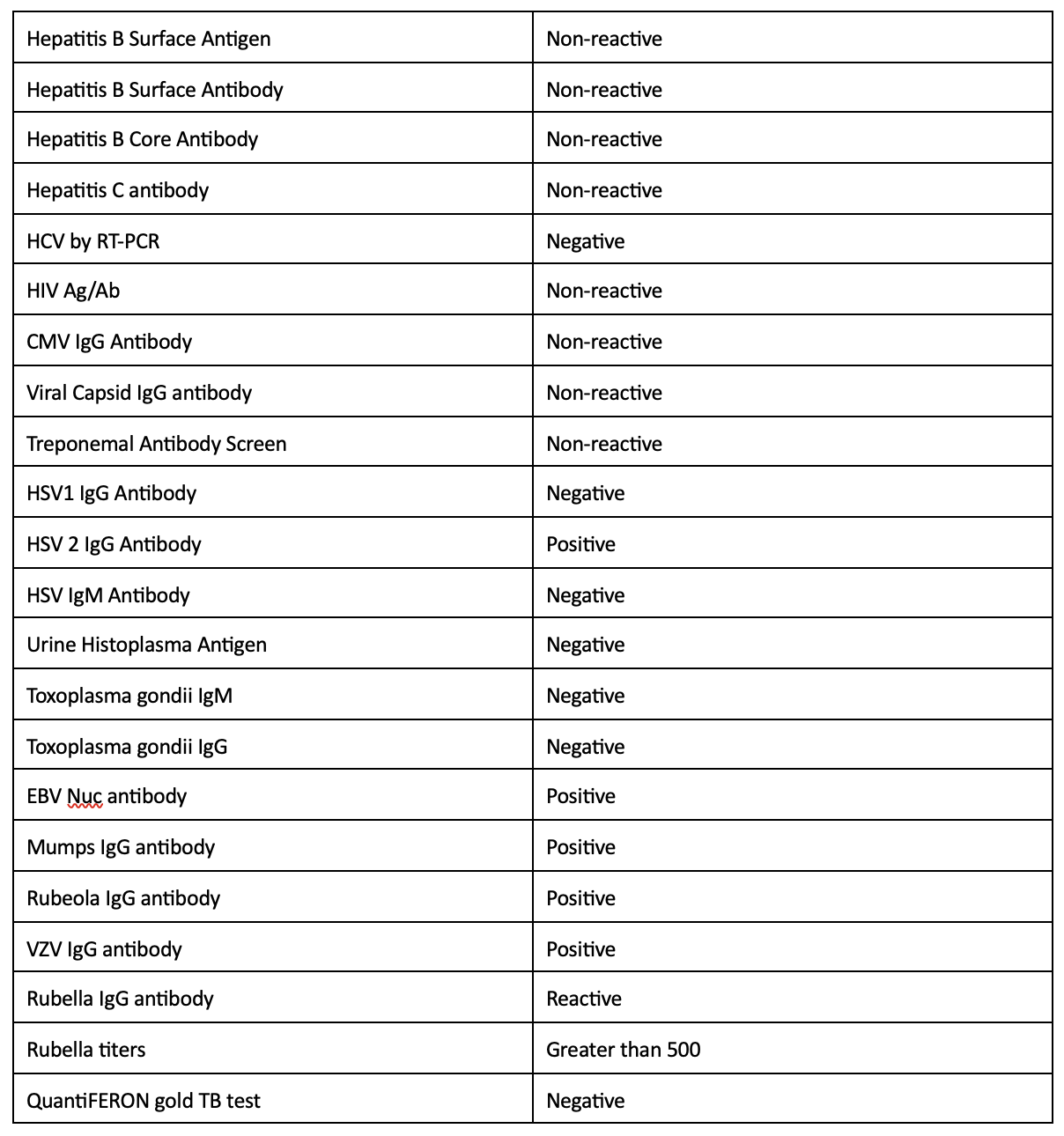
Methods: A 66-year-old male with a history of non-ischemic cardiomyopathy and atrial fibrillation (AF) presented to the hepatology outpatient clinic for pre-heart transplant evaluation to discuss liver biopsy findings. The liver biopsy demonstrated non-necrotizing granulomas (NNG) in portal tract, scattered microgranulomas in lobules and portal and periportal fibrosis without cirrhosis. He denied any significant alcohol use, recreational drug use or prior known liver disease. He had no history of travel outside the US. He denied a family history of liver disease or sarcoidosis. Of note, he had been on amiodarone 200mg daily for more than 5 years for his AF complicated by multiple episodes of ventricular tachycardia. An infectious work-up was unremarkable, Table 1. Autoimmune work-up included anti-mitochondrial antibody and ACE level, both of which were in negative. Given the unremarkable work-up, the NNG were attributed to amiodarone use. At his cardiology pre-transplant clinic, he was transitioned from amiodarone to quinidine. Discussion: In Western countries, leading cause of GH is autoimmune liver diseases such as primary biliary cholangitis while infections remain a predominant cause in regions with higher prevalence of tuberculosis. Idiopathic GH accounts for a minority of cases. Several studies have noted an association between amiodarone-associated bone marrow granulomas. The pathophysiology involves the buildup of the drug and its metabolites in lysosomes of macrophages, leading to phospholipidosis and resulting in cellular injury. This process activates inflammasomes, which drive a localized inflammatory response to promote granuloma formation. With this mechanism amiodarone can cause NNGs to form in multiple organs. Treatment of GH involved treating the underlying cause as seen in a literature review, where amiodarone was stopped in 5 cases with improvement in 3 of the cases. This case highlights the importance of recognizing drug-induced granulomatous hepatitis as a potential adverse effect of amiodarone therapy.