Lauren Davis, DO, Erin Hollis, DO, Mark McGarrey, MD, Julianna Tantum, DO, Nicole Albert, DO Lankenau Medical Center, Wynnewood, PA Introduction: Granulomatous liver disease can have several etiologies, and non-caseating granulomas are commonly associated with sarcoidosis or autoimmune disease. We present a patient with respiratory symptoms and elevated liver enzymes who was found to have non-caseating granulomas on biopsy due to disseminated Mycobacterium chelonae.
Case Description/
Methods: A 68-year-old male with prior latent tuberculosis presented with a cough following viral respiratory infection. CT chest revealed a right lower lobe calcified granuloma. Liver enzymes were incidentally elevated with AST 97 IU/L, ALT 63 IU/L, ALP 387. Workup included negative hepatitis panel, HIV, and autoimmune serologies.He underwent a liver biopsy revealing nonspecific inflammation with non-necrotizing portal tract and lobular granulomata, concerning for granulomatous hepatitis (Figure 1). He was referred to Infectious Disease and underwent a full viral, parasitic, and fungal workup, including sputum culture, which was initially unrevealing. He was referred to a liver center for additional workup. Meanwhile, he underwent bronchoscopy with pulmonology but developed respiratory distress and hemodynamic instability post-procedure requiring intubation and admission. While hospitalized, his outpatient sputum cultures resulted with evidence of Mycobacterium chelonae. He started on IV Imipenem, Clarithromycin, and Tobramycin for suspected disseminated Mycobacterium. Unfortunately, he had further deterioration from septic shock and respiratory failure and ultimately passed despite treatment. Discussion: Disseminated disease due to M chelonae is rare, with approximately 100 cases reported. In our case, elevated liver enzymes were the first clue that led to further investigation and the identification of granulomatous hepatitis. Granulomatous hepatitis has a wide differential that includes infectious, autoimmune, and drug-induced causes. While mycobacterial infectionsare well-known etiologies, typically causing necrotizing granuloma, M. chelonae is rarely implicated. The absence of systemic signs at presentation, the subacute course, and presence of non-caseating granuloma further complicated this diagnosis. In this case, the identification of innumerable non-necrotizing granulomas on liver biopsy, despite negative acid-fast staining, prompted a thorough infectious evaluation, ultimately leading to the diagnosis. Early recognition and multidisciplinary evaluation are critical to diagnosis and management, although outcomes may remain poor despite therapy.
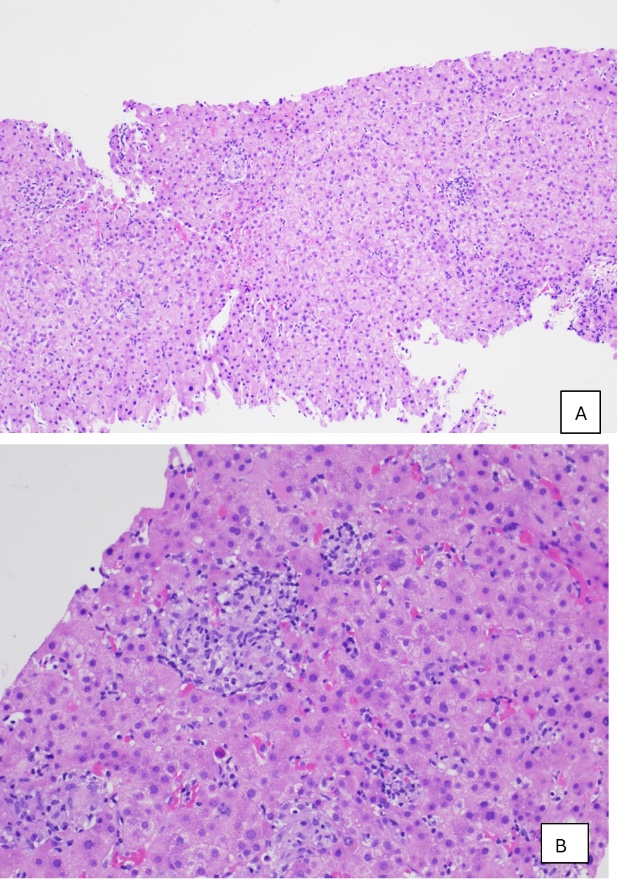
Figure: Figure 1: Pathology for liver biopsy showing 10x magnification (A) and 20x magnification (B) with evidence of non-caseating granuloma suggestive of granulomatous hepatitis.
Disclosures: Lauren Davis indicated no relevant financial relationships. Erin Hollis indicated no relevant financial relationships. Mark McGarrey indicated no relevant financial relationships. Julianna Tantum indicated no relevant financial relationships. Nicole Albert indicated no relevant financial relationships.
Lauren Davis, DO, Erin Hollis, DO, Mark McGarrey, MD, Julianna Tantum, DO, Nicole Albert, DO. P1877 - Disseminated Mycobacterium Chelonae: A Rare Cause of Non-caseating Granulomatous Hepatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.