Anudeep Jala, DO1, Daniel Moodey, DO2, Sachin Prasad, DO3, Seth Lipshutz, DO4, Christopher Chhoun, DO1, Drew Chiesa, DO5 1Jefferson Health, Voorhees, NJ; 2Jefferson Health, Somerdale, NJ; 3Jefferson Health, Blackwood, NJ; 4Jefferson Health, Cherry Hill, NJ; 5Jefferson Health, Sewell, NJ Introduction: Liver abscesses typically occur from hematogenous dissemination of intra-abdominal infections or from infections originating from the biliary tract. Sources of intra-abdominal infections include, but are not limited to, diverticulitis and inflammatory colitis with spread to the liver via the portal venous system. Biliary infections, such as cholecystitis and cholangitis, are also well-documented causes of liver abscesses. Less common causes include parasitic and fungal pathogens. Other risk factors for liver abscesses include diabetes, end-stage renal disease, cirrhosis, and malignancy. We present a rare case of a liver abscess with no apparent infectious source or traditional risk factors.
Case Description/
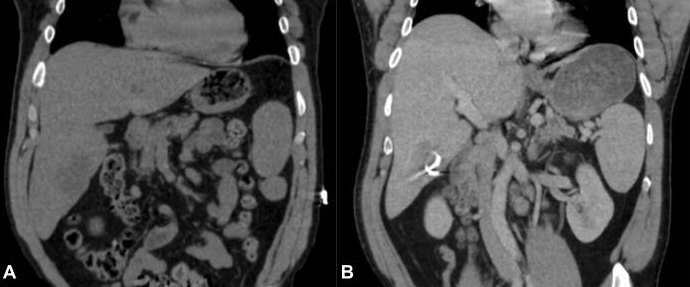
Methods: A 55-year-old male with a medical history of Beckwith-Wiedemann syndrome and nephrolithiasis initially presented to the hospital for evaluation of fevers, chills, and body aches. Initial workup included computed tomography (CT) of the abdomen, which demonstrated a 6.3 cm multiloculated hepatic abscess. The biliary system was unremarkable, with no evidence of cholelithiasis or biliary obstruction and a normal common bile duct diameter.
The patient had undergone percutaneous drainage of the abscess with catheter placement by interventional radiology. Culture of the hepatic abscess returned with anaerobic gram-negative rods. Blood cultures remained negative throughout the hospitalization. Given the unclear etiology, a liver biopsy was recommended to rule out malignancy, and an outpatient colonoscopy was planned following completion of antibiotic therapy. Discussion: This case is notable due to the absence of a clear infectious source or predisposing risk factors. While Beckwith-Wiedemann syndrome is not currently associated with hepatic abscess formation, it may warrant further investigation in such unusual presentations. Complications of intrahepatic abscess can include pleural empyema, portal vein thrombosis, and rupture into adjacent cavities. This case demonstrates the importance of maintaining a broad differential diagnosis and considering hepatic abscesses in patients without classical risk factors.
Figure: Figure 1: (A) CT abdomen revealing a hypodense lesion within the inferior aspect of the right hepatic lobe, (B) Placement of pigtail catheter for percutaneous drainage of the abscess.
Disclosures: Anudeep Jala indicated no relevant financial relationships. Daniel Moodey indicated no relevant financial relationships. Sachin Prasad indicated no relevant financial relationships. Seth Lipshutz indicated no relevant financial relationships. Christopher Chhoun indicated no relevant financial relationships. Drew Chiesa indicated no relevant financial relationships.
Anudeep Jala, DO1, Daniel Moodey, DO2, Sachin Prasad, DO3, Seth Lipshutz, DO4, Christopher Chhoun, DO1, Drew Chiesa, DO5. P1830 - A Mystery Within: Idiopathic Intrahepatic Abscess in the Absence of Traditional Risk Factors, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpeg.jpg "Anudeep Jala, DO (he/him/his) photo")