Ballad Health - Richmond, VA UNITED STATES - Richmond, VA Norton, VA
Award: ACG Presidential Poster Award
Rafi Iftekhar, MD1, Usama Abu-Heija, MBBS2, Ahmad Hmidat, MD2, Maya Shatta, MBBS3, Noah Hall, MD4 1Ballad Health - Richmond, VA UNITED STATES - Richmond, VA, Norton, VA; 2East Tennessee State University, Johnson City, TN; 3statcare, Knoxville, TN; 4Mountain Home VA Medical Center, Jonesborough, TN Introduction: Ascites is commonly linked to hepatic, malignant, or infectious causes. However, when ascitic fluid characteristics are atypical, bladder rupture—though rare—should be considered. We present a case of spontaneous intraperitoneal bladder rupture mimicking portal hypertensive ascites to underscore the need to include urologic etiologies in the differential.
Case Description/
Methods: A 73-year-old man with a history of non-Hodgkin’s lymphoma, hypertension, Obstructive Sleep Apnea, atrial flutter, and Post Traumatic Stress Disorder, presented with four days of sharp epigastric pain radiating to the lower quadrants, nausea, vomiting, constipation, and reduced urine output. He denied NSAID use or similar prior symptoms.
Labs showed severe Acute Kidney Injury (creatinine 17.6 mg/dL from baseline ~1), leukocytosis, pyuria, hematuria, and elevated C-Reactive Protein. Liver enzymes and lipase were unremarkable. CT abdomen revealed new moderate-volume ascites and presacral fluid. Paracentesis drained several liters of ascitic fluid with high SAAG ( >1.1 g/dL) and low protein (< 2.5 g/dL), suggestive of portal hypertension and initially raising concern for cirrhosis.
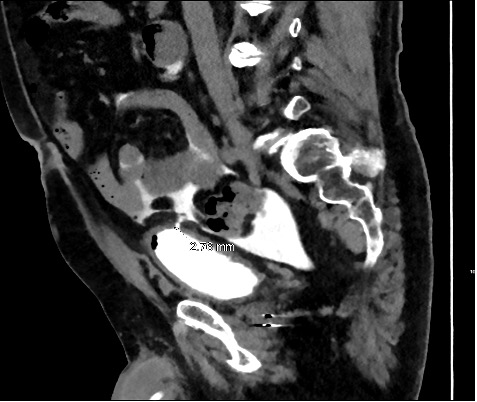
However, post-paracentesis imaging revealed pneumoperitoneum—unexpected in portal hypertension—prompting CT cystogram, which demonstrated a 3 mm dome rupture of the bladder (Figure-1). This explained both the urinary ascites and free air. No obstruction or retroperitoneal extension was seen. Urology performed successful robotic bladder repair (Figure 2). Discussion: Spontaneous intraperitoneal bladder rupture is rare and can mimic hepatic or gastrointestinal pathology. In this case, ascitic fluid findings suggested portal hypertension, leading to initial misclassification. Pneumoperitoneum, unusual for bladder rupture, was a critical clue. The bladder dome is intraperitoneal, so rupture permits urine and gas to enter the peritoneum.
Additionally, peritoneal absorption of urinary creatinine can falsely elevate serum creatinine, simulating intrinsic AKI. This patient’s renal function rapidly improved after surgical repair, supporting this mechanism. Recognizing this rare entity requires high suspicion when fluid analysis and imaging conflict. Timely diagnosis and multidisciplinary care are essential to avoid complications like chemical peritonitis and renal failure. Multidisciplinary collaboration was pivotal to this patient's care.
Figure: Figure-1
Figure: Figure-2
Disclosures: Rafi Iftekhar indicated no relevant financial relationships. Usama Abu-Heija indicated no relevant financial relationships. Ahmad Hmidat indicated no relevant financial relationships. Maya Shatta indicated no relevant financial relationships. Noah Hall indicated no relevant financial relationships.
Rafi Iftekhar, MD1, Usama Abu-Heija, MBBS2, Ahmad Hmidat, MD2, Maya Shatta, MBBS3, Noah Hall, MD4. P1820 - When the Bladder Breaks: A Rare Leak Leading to Intraperitoneal Ascites, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.