Saurav Kini, MBBS1, Benjamin Hoffmann, MD1, Simardeep Singh, MBBS2, Anjali Rajagopal, MBBS3, Frederic Gordon, MD1 1Tufts Medical Center, Boston, MA; 2MedStar Georgetown University Hospital, Baltimore, MD; 3University of Connecticut, Hartford, CT Introduction: Disseminated VZV resulting in hepatitis and central nervous system (CNS) involvement is exceptionally rare in immunocompetent patients. Varicella pneumonitis as a complication of chickenpox is well described in adults. Most cases of dissemination in literature have occurred in immunocompromised adults. We present a case of hepatitis and multi-organ failure from primary VZV infection in an immunocompetent adult that led to significant morbidity and near mortality.
Case Description/
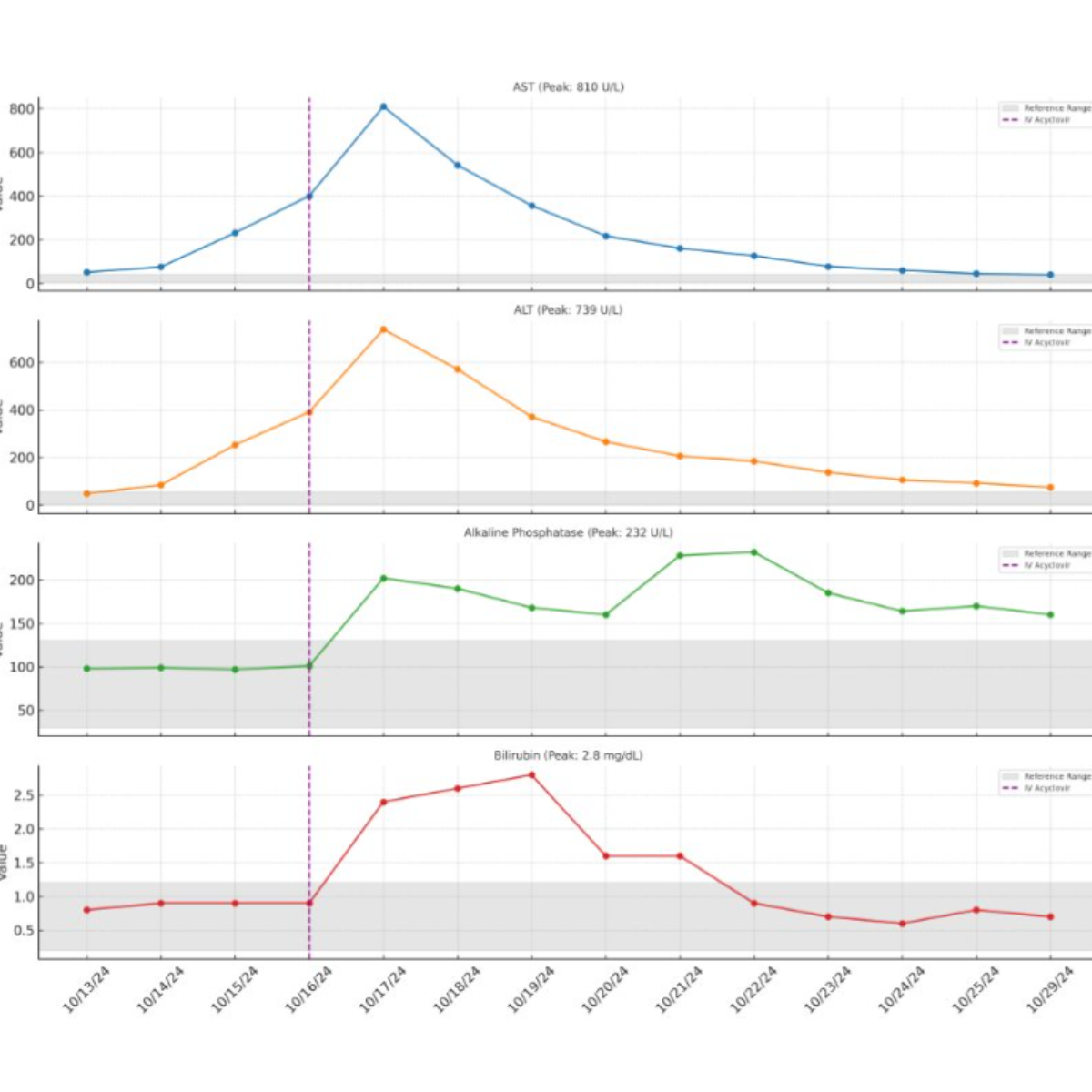
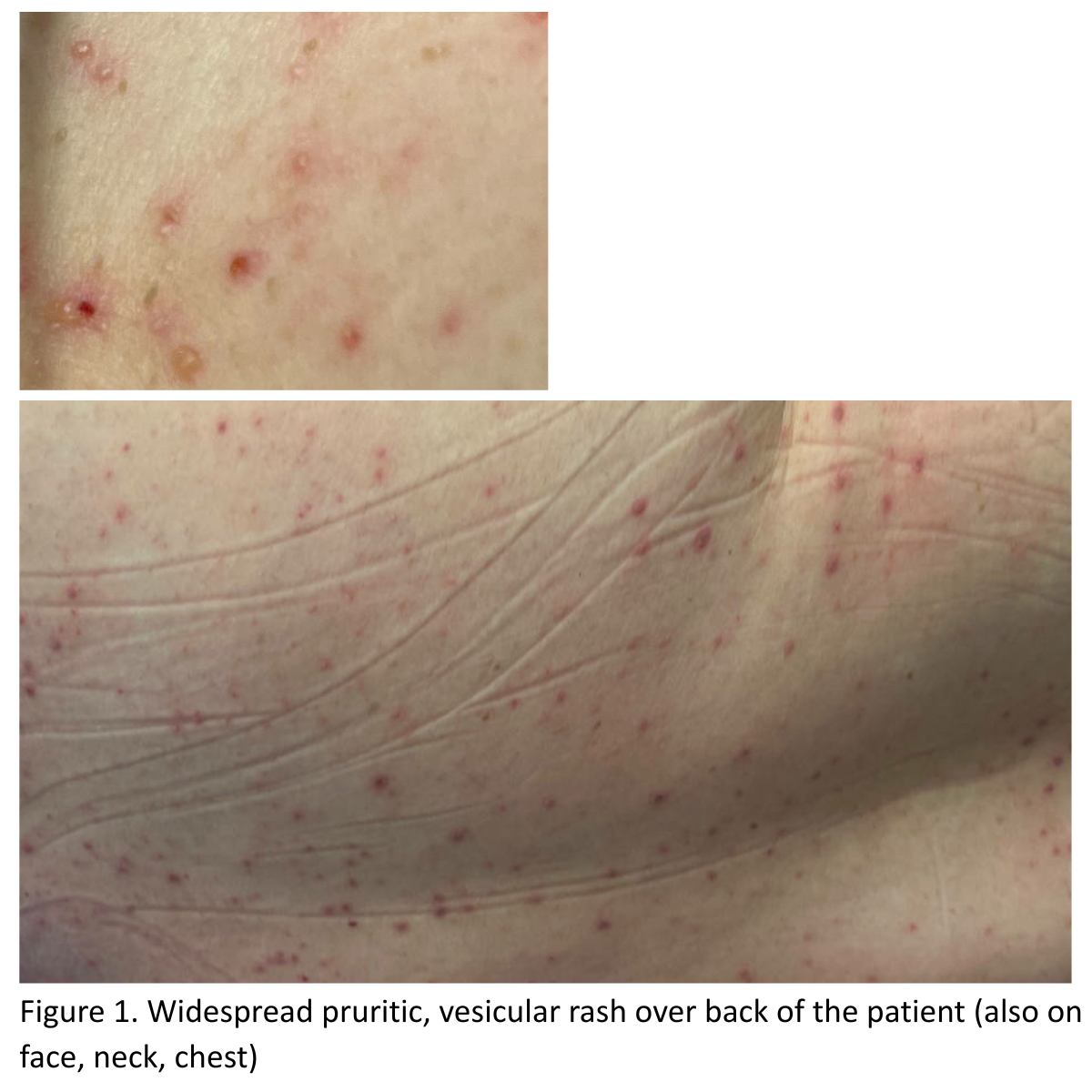
Methods: A 55-year-old immunocompetent female with prior treated hepatitis C presented with epigastric pain, nausea, and vomiting and was found to have CBD dilation and a stone on MRCP for which she underwent an ERCP which was uneventful. On hospital day 3, she developed a diffuse vesicular rash, fevers, and severe abdominal pain in the background of her husband having a primary VZV infection 3 weeks prior, for which valacyclovir was started orally. She had no prior history of immunosuppression, and her testing (including HIV) was suggestive of an immunocompetent adult. She was not vaccinated for primary VZV or shingles. She subsequently developed an acute liver injury, worsening mental status requiring intubation and ICU transfer. IV acyclovir as well as N-acetylcysteine (NAC) was started. Testing of the rash (figure 1) and lumbar puncture confirmed VZV PCR positive, which confirmed disseminated VZV infection. On admission, her liver function was within normal limits with no prior chronic liver disease. Liver injury peaked on day 4 (AST 860 U/L, ALT 746 U/L, ALP 207 U/L, total bilirubin 2.3 mg/dL, INR 1.43, Graph 1 for trend). Her clinical course improved upon starting IV Acyclovir, and a liver biopsy was deferred. She was extubated after 96 hours. Liver enzymes normalized on day 16 of admission. Discussion: Disseminated primary VZV is exceedingly rare in immunocompetent adults but can lead to fulminant hepatitis, encephalitis, and multiorgan failure. Although she had a history of hepatitis C that was treated, she had no other infections suggestive of an immunocompromised state. The collateral history from her husband was crucial in clinching the diagnosis. This also highlights the need for early viral PCR testing (VZV, HSV) of rashes in adults with unexplained hepatitis and neurological symptoms, as well as prompt initiation of IV acyclovir and NAC which may improve outcomes. The rapid progression with high morbidity underscores the importance of prompt recognition and maintaining a high index of suspicion.
Figure: Figure 1. Widespread pruritic, vesicular rash over back of the patient (also on face, neck, chest)
Figure: Graphic trend of Liver function testing highlighting the peak and subsequent improvement after starting Acyclovir
Disclosures: Saurav Kini indicated no relevant financial relationships. Benjamin Hoffmann indicated no relevant financial relationships. Simardeep Singh indicated no relevant financial relationships. Anjali Rajagopal indicated no relevant financial relationships. Frederic Gordon indicated no relevant financial relationships.
Saurav Kini, MBBS1, Benjamin Hoffmann, MD1, Simardeep Singh, MBBS2, Anjali Rajagopal, MBBS3, Frederic Gordon, MD1. P1774 - When Chickenpox Turns Deadly: Acute Hepatitis and Multi-Organ Failure From Primary VZV in an Immunocompetent Adult, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Saurav Kini, MBBS photo")