University of Pittsburgh Medical Center Pittsburgh, PA
Justin-James Chua, MD, Kseniya Anishchenko, MD, Jerome Givi, MD, MPH, Albert Ha, MD, Stela Celaj, MD, PhD University of Pittsburgh Medical Center, Pittsburgh, PA Introduction: Nodular regenerative hyperplasia (NRH) is a rare cause of non-cirrhotic portal hypertension characterized by a widespread hepatic parenchymal transformation into benign regenerative nodules. Its prevalence is unclear, with one European study diagnosing 4% of all liver biopsies with NRH and more recent literature highlighting increasing recognition with more than several hundred NRH cases worldwide in the past few decades. We report on a patient with histologically proven NRH and cryptogenic cirrhosis complicated by chronic portal vein thrombosis (PVT) and significant portal hypertension necessitating transsplenic portal vein recanalization (PVR) and transjugular intrahepatic portosystemic shunt (TIPS).
Case Description/
Methods: A 20-year-old man with medical history of NRH and cryptogenic cirrhosis presented to the hospital for hemodynamically significant hematemesis. Labs were notable for Hgb 10.2 g/dL (baseline 14 g/dL), PLT 91 x 109/L, MELD 3.0 score of 10. A contrasted CT scan demonstrated a chronic PVT and massive hepatosplenomegaly with significant gastroesophageal and splenorenal venous collaterals. Subsequent esophagogastroduodenoscopy (EGD) revealed 2 large columns of esophageal varices that were banded, as well as type 2 gastroesophageal varices with a fibrin plug suggesting likely recent bleed (Figure 1). He had recurrent large hematemesis requiring urgent trans-splenic PVR for chronic PVT followed by TIPS. The hepatic venous portal gradient was reduced from 19 mmHg to 4 mmHg, however with a persistent large gastrorenal venous shunt. Repeat EGD revealed persistent large esophageal and type 2 gastroesophageal varices. An abdominal duplex ultrasound noted a patent TIPS. Given TIPS patency, coil occlusion of the gastrorenal shunt and antegrade embolization of both esophageal and gastric varices was done. He was subsequently discharged home in stable condition. Discussion: There is a paucity of literature on simultaneous NRH and cryptogenic cirrhosis. This case highlights this rare occurrence with complications of clinically significant portal hypertension with extensive portosystemic collaterals. It further underscores the need for a multidisciplinary management strategy, integrating both endoscopic and interventional radiologic approaches.
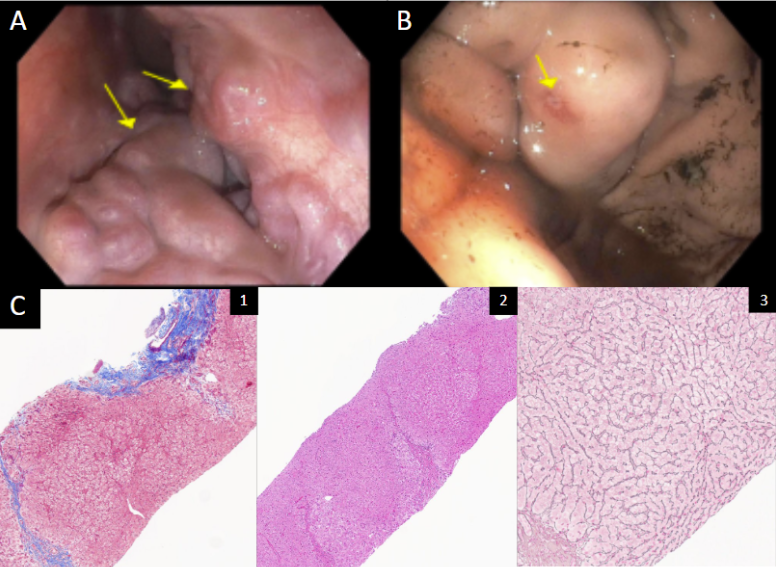
Figure: Figure 1: A.) Initial EGD visualizing 2 large columns of grade III esophageal varices. B.) Initial EGD visualizing type 2 gastroesophageal varices with fibrin plug. C.) Prior liver biopsy pathology: 1) Trichrome stain (5x) demonstrating F3-4 bridging and sinusoidal fibrosis. 2) H&E stain (3x) demonstrating a vague, ill-defined nodular pattern. 3) Reticulin stain (10x) demonstrating compression of normal parenchyma by nodular hyperplasia.
Disclosures: Justin-James Chua indicated no relevant financial relationships. Kseniya Anishchenko indicated no relevant financial relationships. Jerome Givi indicated no relevant financial relationships. Albert Ha indicated no relevant financial relationships. Stela Celaj indicated no relevant financial relationships.
Justin-James Chua, MD, Kseniya Anishchenko, MD, Jerome Givi, MD, MPH, Albert Ha, MD, Stela Celaj, MD, PhD. P1759 - A Case of Significant Portal Hypertension in Simultaneous Nodular Regenerative Hyperplasia and Cryptogenic Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")