Creighton University School of Medicine Phoenix, AZ
Harrison Chou, BS1, Ericka Charley, MD2, Wael Youssef, MD2, Aida Rezaie, MD2 1Creighton University School of Medicine, Fremont, CA; 2Creighton University School of Medicine, Phoenix, AZ Introduction: Portal hypertension is commonly caused by cirrhosis, but non-cirrhotic mechanisms can also elevate portal venous pressure known as non-cirrhotic portal hypertension (NCPH). NCPH can result from vascular malignancies or hematologic conditions. This includes neoplastic plasma cell dyscrasias like multiple myeloma, and typically have plasma cell infiltration on liver biopsy. Gastric varices are a life threatening complication of portal hypertension and acute liver failure. We present a case of a gastric variceal bleeding in a patient with acute liver failure from multiple myeloma, without commonly described liver biopsy findings.
Case Description/
Methods: A 51 year old man with a history of smoldering multiple myeloma presented for melena for one month and a hemoglobin of 4.7 g/dL. The patient denied any history of cirrhosis, alcohol use, medications or prior liver disease. The patient was never treated with chemotherapy for his multiple myeloma. Esophagogastroduodenoscopy (EGD) revealed large gastric varices with high risk stigmata of bleeding, that subsequently bled during the procedure and was treated with hemospray. The patient underwent urgent transhepatic embolization of the gastric varices. During access to one of the varices, perforation and bleeding occurred and was treated with plug and gelfoam embolization. Computed tomography of the abdomen revealed a patent portal vein and signs of portal hypertension without obvious signs of cirrhosis. Laboratory evaluation revealed pancytopenia, normal clotting time, normal liver enzymes, and hypoalbuminemia. Measurement of the trans-sinusoidal porto-systemic pressure gradient was elevated to 13 mm Hg, confirming portal hypertension. A liver biopsy demonstrated nonspecific mild chronic hepatitis, sinusoidal dilation, and periportal fibrosis. Discussion: This case illustrates a clinically challenging presentation of NCPH in a patient with smoldering multiple myeloma. The presence of periportal fibrosis and sinusoidal dilation suggests the NCPH may be related to sinusoidal injury in multiple myeloma. However, the pathologic process may be patchy, focal or submicroscopic, and not always seen on liver biopsy. Additionally, hepatic failure may result from cytokine induced hepatotoxicity, contributing to liver dysfunction without overt hepatic infiltration on biopsy.
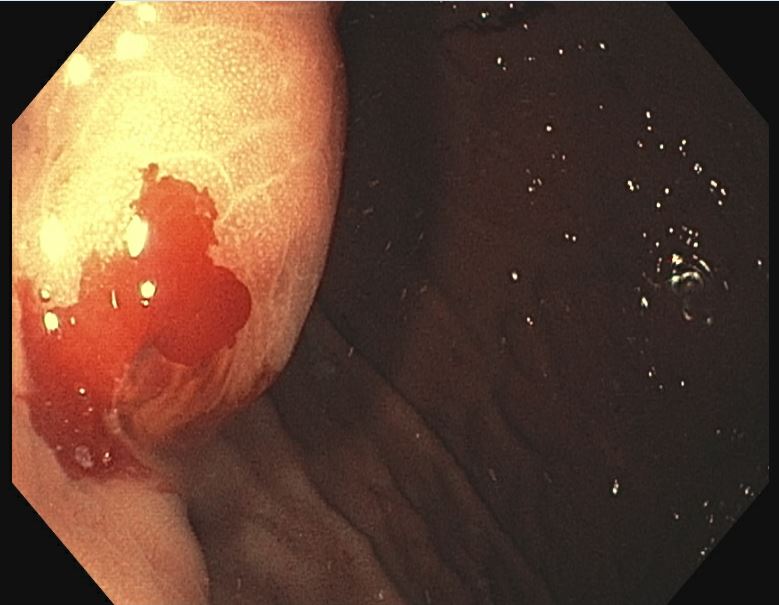
Figure: Pre-embolization Gastric Variceal Bleed in a Patient with Multiple Myeloma
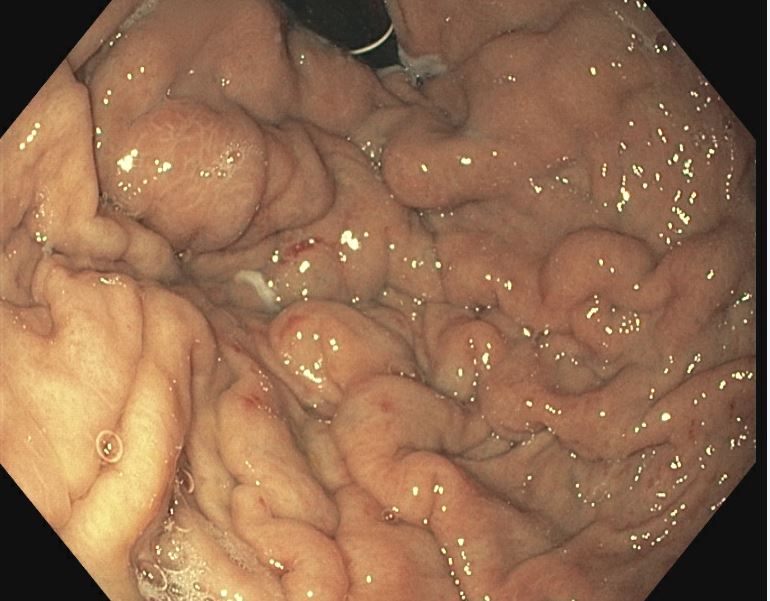
Figure: Post-embolization Gastric Variceal Bleed in a Patient with Multiple Myeloma
Disclosures: Harrison Chou indicated no relevant financial relationships. Ericka Charley indicated no relevant financial relationships. Wael Youssef indicated no relevant financial relationships. Aida Rezaie indicated no relevant financial relationships.
Harrison Chou, BS1, Ericka Charley, MD2, Wael Youssef, MD2, Aida Rezaie, MD2. P1748 - Fulminant Liver Failure in Multiple Myeloma Without Light Chain Deposition Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.