Ochsner University Hospital & Clinics Lafayette, LA
Amit Rajkarnikar, MD1, Jonathan Vignes, MD2 1Ochsner University Hospital & Clinics, Lafayette, LA; 2Ochsner Medical Center, Lafayette, LA Introduction: Hepatopulmonary syndrome (HPS) is characterized by the triad of abnormal arterial oxygenation caused by intrapulmonary vascular dilatations (IPVDs) in the setting of liver disease or portal hypertension. Transthoracic contrast echocardiogram (TTCE) with agitated saline bubble study should be considered for patients with persistent hypoxia and chronic liver disease.
Case Description/
Methods:
69-year-old female with NASH related cirrhosis, splenic and esophageal varices, chronic pancytopenia, T2DM, HLD, remote history of DVT presented with dyspnea on exertion and lightheadedness. Of note, the patient had two prior hospitalizations for atypical chest pain accompanied by shortness of breath in the span of 6 months. She underwent TTCE to assess for intracardiac shunt that demonstrated positive bubble study with evidence of right-to-left shunt physiology, but undetermined if bubbles were early versus late in their timing of shunt. Transesophageal echocardiogram was deferred for concerns of esophageal varices. A second bubble study showed bubbles clearly entering the left atrial cavity through pulmonary veins after 3 cardiac cycles. Bubbles appeared not to cross the atrial wall. This is most consistent with intrapulmonary shunt and with conjunction of underlying cirrhosis HPS was diagnosed. At an initial evaluation with a hepatologist, ABG revealed PaO2 of 61 mm Hg on room air that corrected to 400 mm Hg with 100% FiO2. Repeat ABG two months later showed PaO2 55 mm Hg on room air that improved to 348 mm Hg on 100% FiO2. She met the criteria for moderate to severe Type 1 HPS. She eventually underwent liver transplantation and is doing very well, on room air on follow up.
Discussion: Most patients with HPS present with symptoms and signs of chronic liver disease, that are neither sensitive nor specific for HPS. TTCE with agitated saline is the gold standard for diagnosing pulmonary vascular dilatation. Based on observational studies, liver transplantation demonstrates complete or near complete resolution of HPS with improved oxygenation and shunt in the majority (about 80 percent) of patients within 6 to 12 months. Given the nature of rapid progression and poor prognosis, it is crucial to have a high suspicion for HPS in a patient with liver disease and hypoxia for prompt referral for liver transplant evaluation.
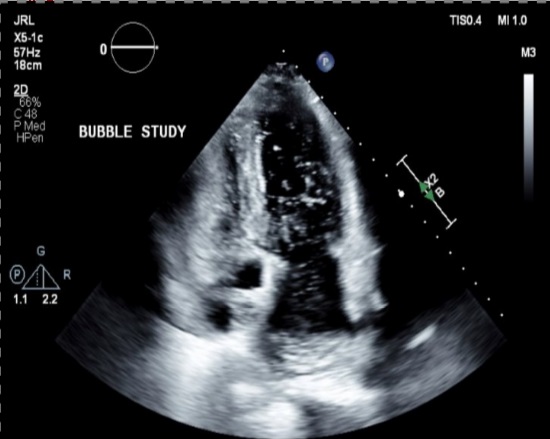
Figure: Transthoracic contrast echocardiogram showing bubbles clearly entering left atrial cavity through pulmonary veins.
Figure: CTA chest noted with hepatosplenomegaly and splenic varices.
Disclosures: Amit Rajkarnikar indicated no relevant financial relationships. Jonathan Vignes indicated no relevant financial relationships.
Amit Rajkarnikar, MD1, Jonathan Vignes, MD2. P1685 - Hepatopulmonary Syndrome Ought to Be Considered in Patients With Chronic Liver Disease and Persistent Hypoxia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")