P1481 - Endoscopic Management of Iatrogenic Type 1 Duodenal Perforation Using Off-Label Fully Covered Esophageal Self-Expandable Metallic Stent: A Case Report and Review
University of Massachusetts Chan Medical School - Baystate Health Enfield
Herisha Shah, DO, MS1, Tushaar V. Shrimanker, MD, MRCP2, Syed Hamza Sohail, MD3, John Miller, Jr., MD4 1University of Massachusetts Chan Medical School - Baystate Health, Enfield, CT; 2University of Massachusetts Chan Medical School-Baystate Medical Center, Enfield, CT; 3University of Massachusetts Chan Medical School - Baystate Health, Springfield, MA; 4University of Massachusetts Chan Medical School-Baystate Medical Center, Springfield, MA Introduction: Duodenal perforation is a serious but uncommon complication of endoscopic retrograde cholangiopancreatography (ERCP) [1]. While this is usually managed surgically, this can be a challenge for high-risk surgical patients. We present a case where a novel endoscopic approach using an off-label fully covered esophageal self-expandable metallic stent (FCSEMS) was used to manage a type 1 duodenal perforation.
Case Description/
Methods: A 75-year-old female with pancreatic adenocarcinoma, prior biliary stenting, and many comorbidities was transferred to our facility with severe abdominal pain after a failed elective biliary stent exchange. Imaging revealed a duodenal perforation. Upper endoscopy showed a 4cm full-thickness perforation at the D1/D2 junction. Due to the patient’s poor clinical status, surgical repair was avoided and endoscopic therapy was favored. An 8 mm×10 cm FCSEMS was placed over the wire and fixed proximally using endoscopic suturing and through the scope clips (TTSC). An NJ tube was also placed for enteral feeding. Despite initial clinical improvement, the patient was found to have a persistent leak and an abscess on imaging 2 weeks later. Repeat endoscopy showed stent migration, likely due to duodenal angulation from malignancy. Another 20 mm×8 cm FCSEMS was deployed in a stent-in-stent manner with fixation using endoscopic tacking sutures, endoloop, and clips. The leak resolved on imaging, and the patient tolerated enteral intake.
Both stents were removed without complications 3 months later. Inspection revealed granulation tissue and ulceration but no residual perforation. A repeat ERCP allowed for successful exchange of the biliary stent with a covered metal stent, despite anatomical challenges. Discussion: In select non-surgical candidates with type 1 duodenal perforation, off-label use of esophageal FCSEMS can be a viable option for management. Though not FDA-approved for this indication, esophageal stents can mimic the role of unavailable covered duodenal stents. Stent migration remains a concern, mitigated here by a stent-in-stent strategy. Esophageal FCSEMS may offer a therapeutic option in these complex cases until such time that dedicated duodenal stents are available.
References: [1]. Turner RC, Steffen CM, Boyd P. Endoscopic duodenal perforation: surgical strategies in a regional centre. World J Emerg Surg. 2014;9(1):11. Published 2014 Jan 24. doi:10.1186/1749-7922-9-11
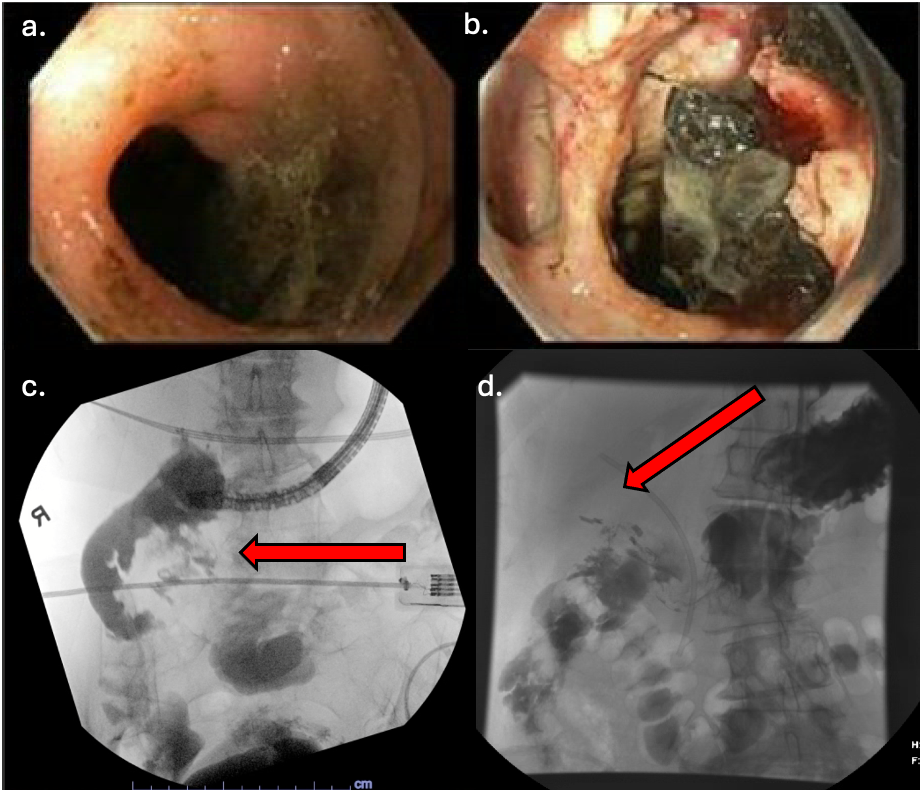
Figure: Figure 1. Duodenal Perforation on Imaging
a. Distal duodenal bulb defect on EGD
b. Necrotic debris in retroperitoneal collection on EGD
c. Duodenal perforation and contrast extravasation on Fluoroscopy
d. Duodenal perforation and contrast extravasation on Fluoroscopy
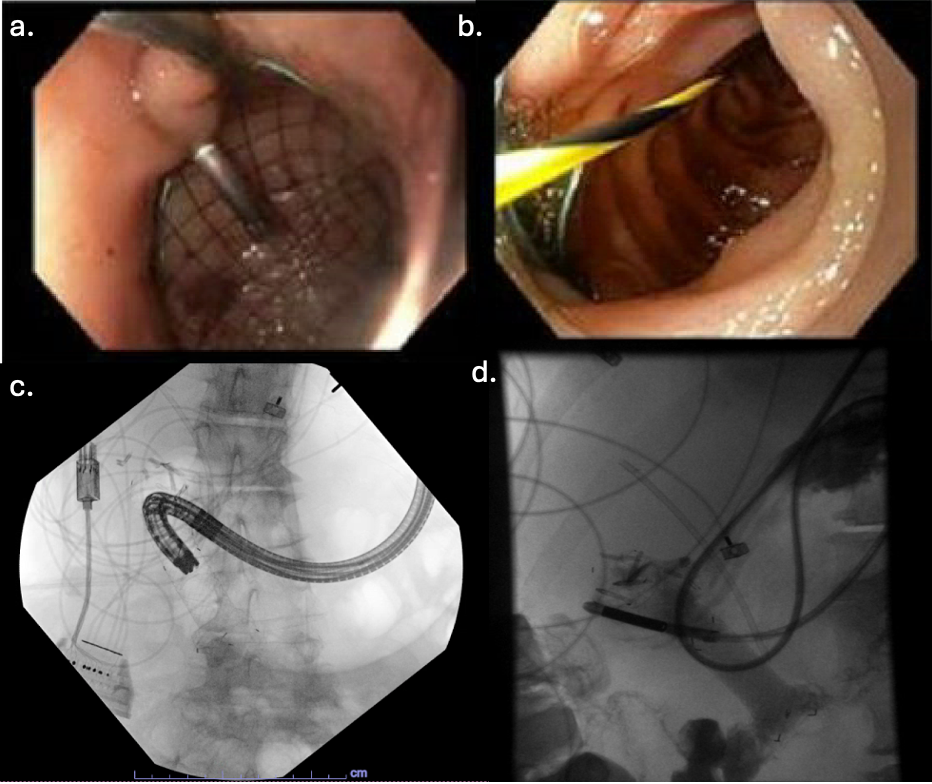
Figure: Figure 2. Esophageal FCEMS on imaging
a. Wire guided insertion of Esophageal FCEMS on EGD
b. Wire guided insertion of Esophageal FCEMS on EGD
c. Esophageal FCEMS in duodenum on Fluoroscopy
d. Esophageal FCEMS in duodenum on Fluoroscopy
Disclosures: Herisha Shah indicated no relevant financial relationships. Tushaar Shrimanker indicated no relevant financial relationships. Syed Hamza Sohail indicated no relevant financial relationships. John Miller, Jr. indicated no relevant financial relationships.
Herisha Shah, DO, MS1, Tushaar V. Shrimanker, MD, MRCP2, Syed Hamza Sohail, MD3, John Miller, Jr., MD4. P1481 - Endoscopic Management of Iatrogenic Type 1 Duodenal Perforation Using Off-Label Fully Covered Esophageal Self-Expandable Metallic Stent: A Case Report and Review, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")