Preeyati Chopra, MBBS1, Khushboo Gala, MD2, Mayank Goyal, MBBS2, Ashwariya Ohri, MBBS3, Ryan Alexander, MD2, Eric J.. Vargas, MD, MS2 1Mayo Clinic, Hartford, CT; 2Mayo Clinic, Rochester, MN; 3Mayo Clinic, Indianapolis, IN Introduction: Gastric Outlet Obstruction (GOO) of the excluded stomach is a rare complication following Roux-en-Y gastric bypass (RYGB) surgery, typically attributed to chronic accumulation of gastric secretions. We describe the diagnostic and therapeutic role of endoscopic ultrasound (EUS)-guided decompression for excluded stomach GOO (eGOO) using a lumen apposing metal stent (LAMS).
Case Description/
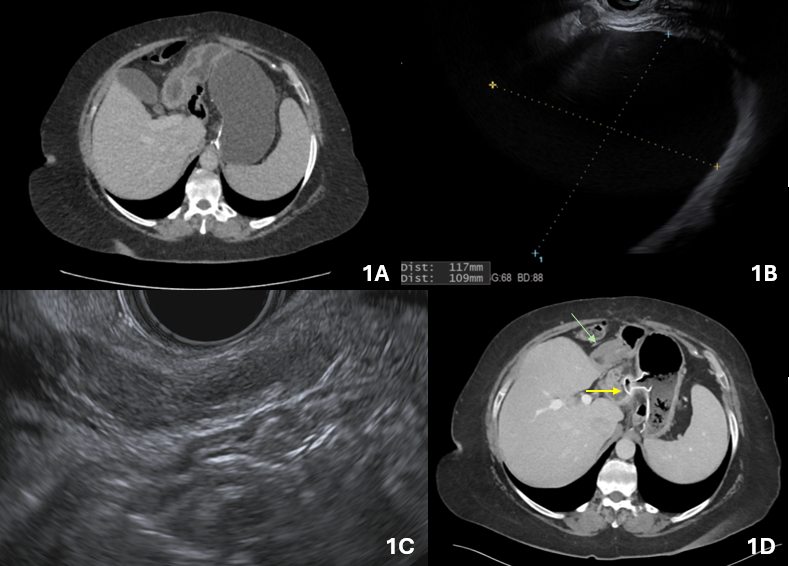
Methods: A 63-year-old female with a history of RYGB (23 years prior) presented with progressive epigastric fullness, nausea, and pain after eating. CT showed significant distension of the excluded stomach representing GOO with non-specific eccentric wall thickening of the gastric antrum (Figure 1A).
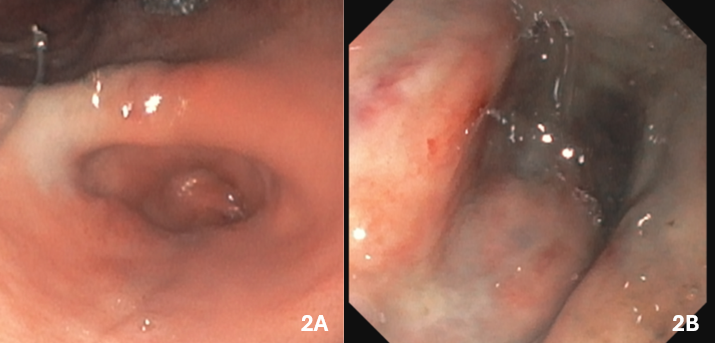
Upper endoscopic evaluation (EGD) was unremarkable. EUS revealed significant distention of the excluded stomach with diffuse wall thickening in the antrum (Figure 1B, 1C). Given these findings, the decision was made to proceed with EUS-directed gastric decompression. A 19-gauge needle was first used to confirm access into the excluded stomach. Using a free-hand technique, a 15 x 10 mm LAMS was used to create a jejuno-gastrostomy between the jejunal saddle and the excluded stomach (Figure 1D). The stent was dilated to 12 mm using a CRE balloon under fluoroscopic guidance to allow for same-session endoscopic evaluation. A slim upper endoscope was introduced through the LAMS into the excluded stomach, and after suctioning >1.5 liters of fluid, pyloric stenosis (Figure 2A) and significant ulceration of the duodenal bulb (Figure 2B) were found. Biopsies confirmed benign peptic ulcer disease with negative H. pylori testing. The patient reported significant improvement in upper GI symptoms thereafter. Subsequent EGD and EUS examinations confirmed benign disease, with repeat imaging in 6 months confirming the absence of neoplasia and complications. Discussion: This case highlights the utility of EUS-directed LAMS placement as both a diagnostic and therapeutic approach for GOO in the excluded stomach. The procedure offers minimally invasive access to an otherwise challenging anatomical location and can provide immediate symptom relief. Given the distinct clinical and anatomical features of this condition, we propose the term excluded stomach gastric outlet obstruction (eGOO) to standardize terminology and facilitate future research and clinical dialogue.
Figure: 1A: CT: GOO of excluded stomach with gastric antral thickening 1B: EUS: Distended excluded stomach 1C: EUS: Non-specific thickening of layer 4 without underlying mass 1D: CT: LAMS between gastric pouch and excluded stomach (yellow arrow), and gastric antral thickening (green arrow)
Figure: Endoscopy through LAMS: Pyloric stenosis (2A) and duodenal bulb ulceration (2B)
Disclosures: Preeyati Chopra indicated no relevant financial relationships. Khushboo Gala indicated no relevant financial relationships. Mayank Goyal indicated no relevant financial relationships. Ashwariya Ohri indicated no relevant financial relationships. Ryan Alexander indicated no relevant financial relationships. Eric Vargas indicated no relevant financial relationships.
Preeyati Chopra, MBBS1, Khushboo Gala, MD2, Mayank Goyal, MBBS2, Ashwariya Ohri, MBBS3, Ryan Alexander, MD2, Eric J.. Vargas, MD, MS2. P1479 - Endoscopic Ultrasound (EUS)-Directed Decompression of Excluded Stomach Gastric Outlet Obstruction (eGOO) After Roux-en-Y Gastric Bypass Surgery, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")