Lauren Davis, DO, Harrison Pajovich, MD, Stefanie Gallagher, DO, MBe, Joseph Triggs, MD Lankenau Medical Center, Wynnewood, PA Introduction: Surgical clip migration is a rare but recognized complication post-cholecystectomy leading to biliary obstruction, stone formation, and cholangitis. Most cases occur within the first few years post-cholecystectomy but delayed presentations can occur. We present a patient with right upper quadrant (RUQ) abdominal pain and markedly elevated liver enzymes, found to have biliary obstruction due to surgical clip migration into the common bile duct (CBD) with secondary choledocholithiasis, 7 years post-cholecystectomy.
Case Description/
Methods: A 64-year-old female with a history of laparoscopic cholecystectomy and Roux-en-Y gastric bypass (RYGB) presented with acute RUQ pain. Labs notable for AST 938 IU/L, ALT 393 IU/L, ALP 259 IU/L, with a normal total bilirubin. RUQ ultrasound showed a dilated CBD of 15 mm without choledocholithiasis. Computed tomography revealed migrated surgical clip in the proximal CBD, which was confirmed by magnetic resonance cholangiopancreatography (Figure 1 and 2). Given the patient's history of RYGB, an endoscopic ultrasound-directed transgastric ERCP (EDGE) was attempted; however, the procedure was aborted due to an inability to distend the collapsed gastric remnant, the first step necessary for the safe creation of the gastrogastric fistula. After multidisciplinary discussion involving interventional gastroenterology and surgery, the decision was to proceed with surgical CBD exploration and stone removal. The patient underwent gastrotomy with intraoperative endoscopy to visualize the ampulla followed by surgical bile duct exploration. Choledochoscopy revealed a 1 cm obstructing stone containing the migrated surgical clip. Both were extracted and a choledochoduodenostomy was created at the site of the choledochotomy. The patient tolerated the procedure, with resolution of her symptoms and improvement in liver enzymes prior to discharge. Discussion: Surgical clip migration is an uncommon but documented cause of biliary obstruction following cholecystectomy. Although the median time to presentation is two years postoperatively, our case highlights that this rare complication can occur many years later. Management of post-cholecystectomy clip-migration is similar to that of non-iatrogenic choledocholithiasis with ERCP as a first-line diagnostic and therapeutic management. Management was further complicated by the patient's altered anatomy due to prior RYGB, demonstrating challenges of post-surgical anatomic variations in the evaluation and treatment of biliary pathology.
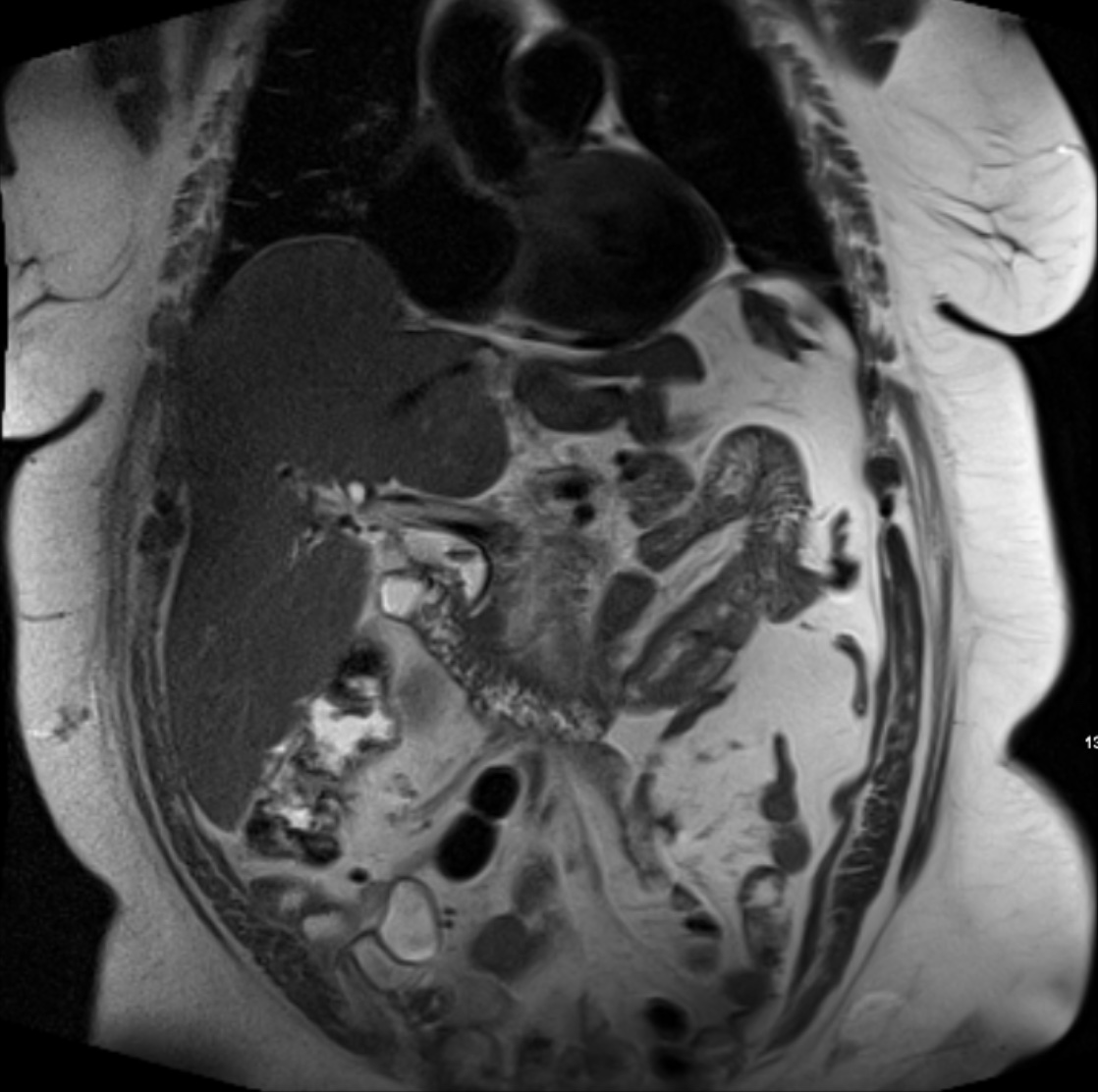
Figure: Figure 1: MRCP T2 Image demonstrating 13mm biliary ductal dilatation with a 7mm linear filling defect within the common bile duct.
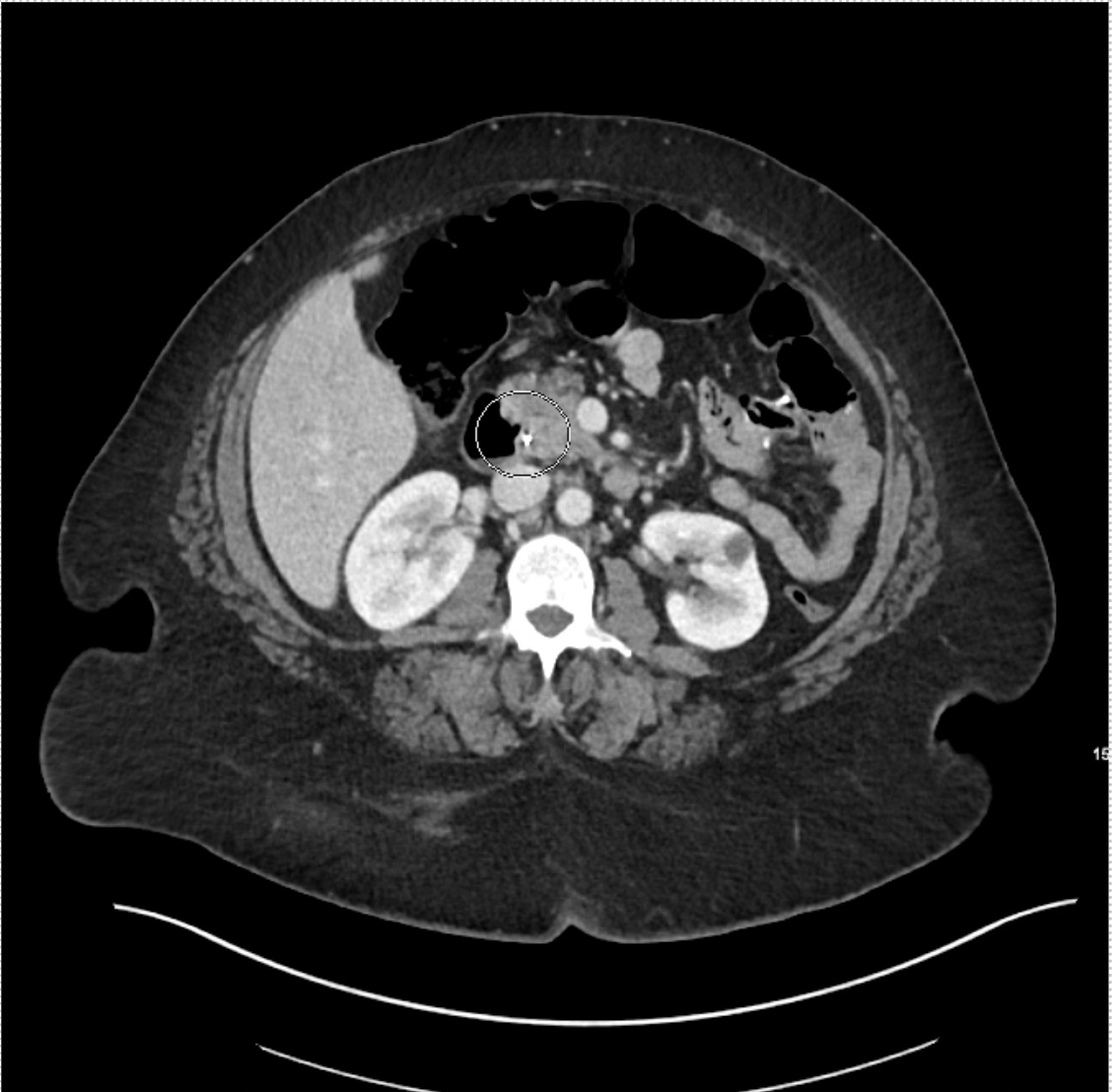
Figure: Figure 2: CT abdomen revealing surgical clip within the proximal common bile duct
Disclosures: Lauren Davis indicated no relevant financial relationships. Harrison Pajovich indicated no relevant financial relationships. Stefanie Gallagher indicated no relevant financial relationships. Joseph Triggs indicated no relevant financial relationships.
Lauren Davis, DO, Harrison Pajovich, MD, Stefanie Gallagher, DO, MBe, Joseph Triggs, MD. P1473 - Wandering Clip: A Rare Case of Post-Cholecystectomy Biliary Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.