University of Texas at Austin Dell Medical School Austin, TX
Noah Fanous, MD1, Mihir Alexander. Patel, MD, MBA1, Deepak Agrawal, MD, MPH2, David Tang, MD1 1University of Texas at Austin Dell Medical School, Austin, TX; 2University of Texas at Austin, Austin, TX Introduction: Afferent Loop Syndrome (ALS) is a relatively uncommon mechanical complication of pancreaticoduodenectomy (~13%). We present a case of ALS due to metastatic duodenal adenocarcinoma resulting in both jejunal and biliary obstruction ultimately treated with endoscopic ultrasound (EUS) guided gastrojejunostomy (GJ) of the obstructed jejunal limb.
Case Description/
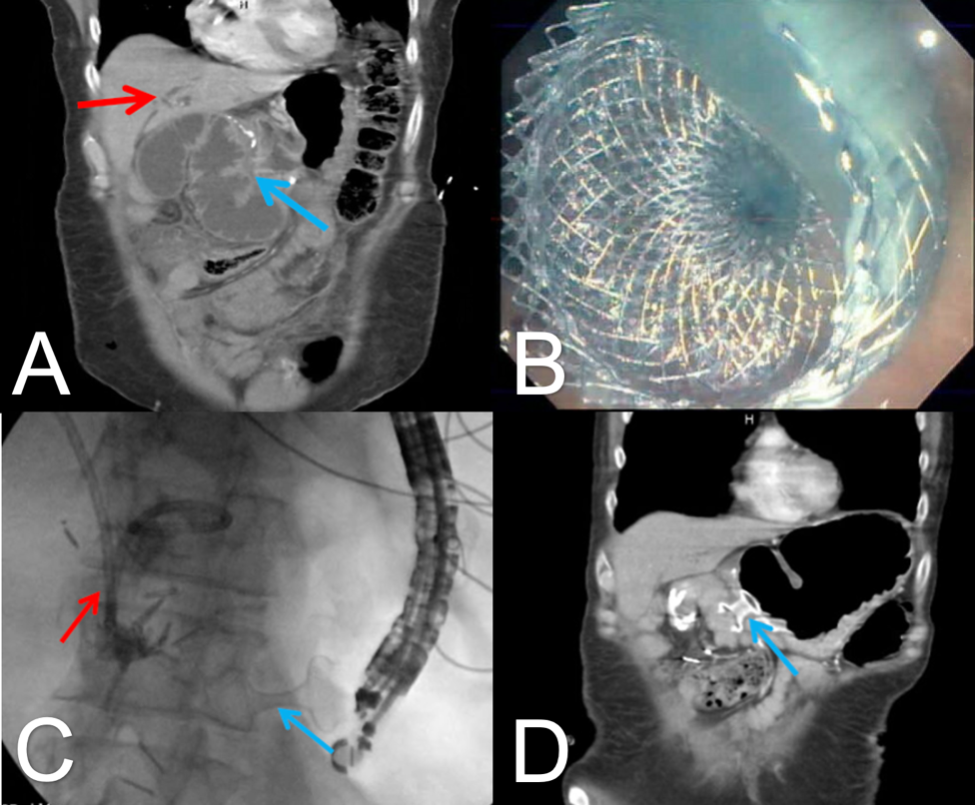
Methods: A 61-year-old male with recent Whipple surgery for pancreatic adenocarcinoma 8 months before and subsequent metastases to liver, lungs, and peritoneum presented with worsening abdominal pain and fever. Laboratory testing included AST 258, ALT 262, ALP 544 units/L, and TBIL 1.9 mg/dL. Abdominal ultrasound noted dilated intra and extrahepatic biliary dilation without choledocholithiasis or obvious hepaticojejunostomy (HJ) stricture. Computed tomography (CT) (Figure 1A) demonstrated biliary dilation and extrinsic compression of the afferent (biliopancreatic) limb consistent with ALS.
On endoscopy, HJ and pancreatojejunostomy were not visualized due to extrinsic jejunal limb narrowing . A 0.035’ wire could not be passed into the afferent or efferent limb precluding placement of a stent. Percutaneous transhepatic cholangiogram with internal-external biliary catheter placement into the distended afferent limb was then performed with improvement in bilirubin and abdominal pain. After discussions with the patient, EUS-guided GJ was offered to remove the external drain and drain the afferent limb into the stomach. Water mixed with methylene blue was then instilled into the afferent limb via the percutaneous biliary drain (PBD). With a linear echoendoscope, the distended afferent limb was easily identified. A 19G FNA needle was used to aspirate the blue fluid to confirm the afferent limb and a 20mm LAMS was deployed. The blue fluid drained from the stent (Figure 1B). LAMS position was confirmed on fluoroscopy (Figure 1C). The external drain was then capped. CT scan two weeks later showed resolution of ALS (Figure 1D). and the external drain was removed. Discussion: EUS-guided GJ was used to treat ALS and ensuing biliary obstruction. We relied on a transhepatic PBD to gain access to the afferent limb. However, if PBD access is not available, the distended afferent limb may be identified on EUS and accessed with a needle. Subsequent contrast infusion into the bowel via needle may be used to confirm access into the closed-loop afferent limb and allow for proper LAMS placement to drain the afferent limb.
Figure: Figure 1: (A) Biliary dilation (red arrow) with extrinsic compression of the afferent (biliopancreatic) limb (blue arrow) at the pancreaticoduodenal tumor bed. (B) Water mixed with methylene blue draining from 20mm LAMS. (C) Fluoroscopic confirmation of deployed LAMS (blue arrow) with percutaneous biliary drain (red arrow). (D)) Internal and external biliary stent with decreased biliary dilatation, distal cystgastrectomy stent in place (blue arrow)
Disclosures: Noah Fanous indicated no relevant financial relationships. Mihir Patel indicated no relevant financial relationships. Deepak Agrawal indicated no relevant financial relationships. David Tang indicated no relevant financial relationships.
Noah Fanous, MD1, Mihir Alexander. Patel, MD, MBA1, Deepak Agrawal, MD, MPH2, David Tang, MD1. P1440 - Gastrojejunostomy with Lumen-Apposing Metal Stent for Afferent Loop Syndrome in Duodenal Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.