Ronan Allencherril, MD, Apaar Dadlani, MD, Scott Berger, MD, Thomas R. McCarty, MD, MPH, Eamonn M.. Quigley, MD, MACG Houston Methodist Hospital, Houston, TX Introduction: Non-steroidal anti-inflammatory drugs (NSAIDs) are a well-known cause of strictures in the gastrointestinal tract. Rare cases of severe strictures have been reported, with delayed passage of even liquid oral intake. Such significant stenoses typically require serial balloon dilations over the course of weeks to months. Lumen-apposing metal stents (LAMS) have demonstrated multiple uses since their introduction over the past few years. Here we present a case of a severe duodenal stricture successfully treated with a LAMS.
Case Description/
Methods: A 48-year-old female with a history of treated H. Pylori, hyperlipidemia, and metabolic associated fatty liver disease presented to clinic with post prandial right upper quadrant pain, associated with bloating, nausea, and vomiting. She reported chronic daily NSAID use.
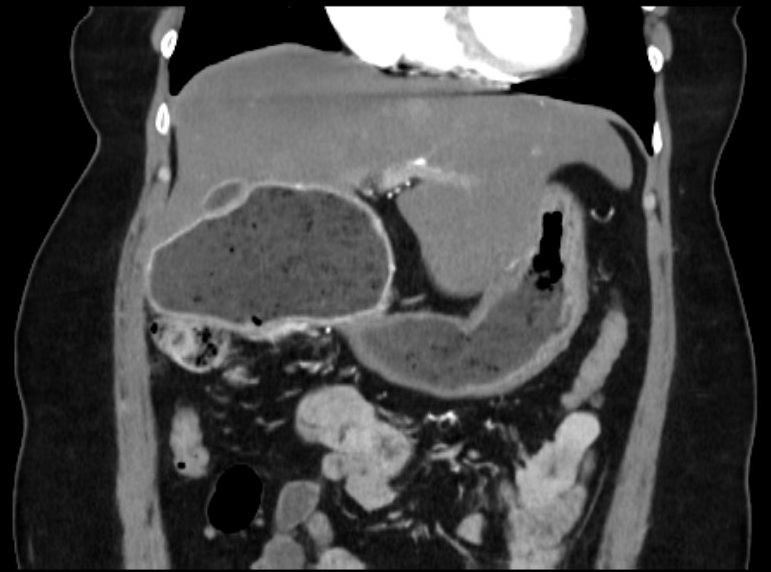
Vitals and basic labs were normal. Computed tomography (CT) of the abdomen showed moderate to high grade duodenal obstruction between D2 and D3 with upstream dilation of the stomach and proximal duodenum (Figure 1). No mass was seen. The common bile duct (CBD) was mildly dilated at 7 mm. Magnetic resonance cholangiopancreatography showed a CBD of 9 mm and a similar duodenal dilation. Given the patient’s country of origin, Trypanosoma cruzi antibodies were ordered and returned negative.
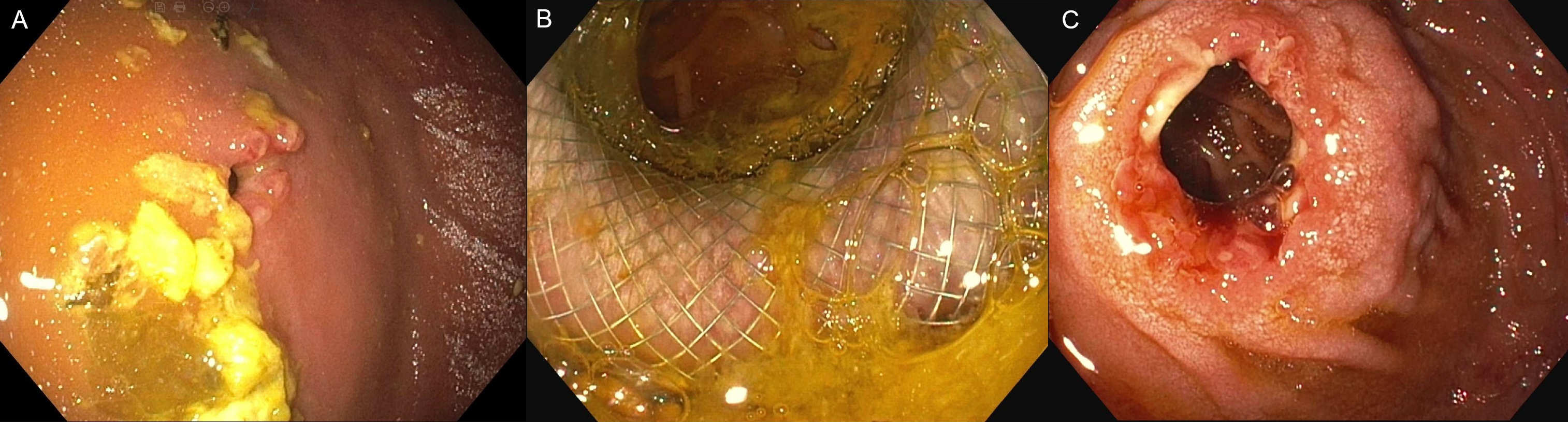
Esophagogastroduodenoscopy (EGD) showed a large amount of gastric contents and marked distension of the duodenal bulb due to severe D2 stenosis (Figure 2A) which could not be traversed despite switching to a pediatric colonoscope and dilating with a through-the-scope balloon to 10 mm. Stricture biopsies showed peptic duodenitis, ulceration, granulation tissue, and fungal yeasts and bacterial rods which were likely contaminants. Immunostains for H. pylori, herpes simplex virus, and cytomegalovirus were negative. She returned for repeat EGD with endoscopic ultrasound (EUS) the following week. A 20x10mm LAMS was placed and dilated with a through-the-scope balloon to 16.5 mm (Figure 2B). EUS exam was limited due to duodenal dilation. The next month, the LAMS was removed and the stricture was dilated to 20 mm. She could tolerate oral intake and has not required further dilations since. Discussion: This case shows an interesting presentation of NSAID induced duodenal stricture. When particularly severe, these strictures can be challenging to dilate. The utilization of LAMS effectively treated the stricture, potentially decreasing the number of repeat dilations needed.
Figure: CT abdomen and pelvis showing moderate to high grade duodenal obstruction at D2/D3 with severe upstream dilation of proximal duodenum.
Figure: 2A: Severe stricture at D2 pre-dilation. 2B: Stricture status post LAMS and balloon dilation. 2C: Stricture status post LAMS removal
Disclosures: Ronan Allencherril indicated no relevant financial relationships. Apaar Dadlani indicated no relevant financial relationships. Scott Berger indicated no relevant financial relationships. Thomas McCarty: Covidien/Medtronic – Consultant. Endoquest Robotics – Consultant. Eamonn Quigley: Food Marble – Advisor or Review Panel Member.
Ronan Allencherril, MD, Apaar Dadlani, MD, Scott Berger, MD, Thomas R. McCarty, MD, MPH, Eamonn M.. Quigley, MD, MACG. P1437 - Severe NSAID-Induced Duodenal Stricture Dilated With Lumen-Apposing Metal Stent, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.