HCA Healthcare Kingwood Hospital/University of Houston Spring, TX
Wafa Mehboob, DO1, Bilal Ashraf, MD2, Galvin S. Dhaliwal, MD2, Aakriti Soni, MD2, Ashvin Singh Dhaliwal, MD3, Sushovan Guha, MD, PhD4, Ahmed Ouni, MD4 1HCA Healthcare Kingwood Hospital/University of Houston, Spring, TX; 2HCA Healthcare Kingwood Hospital/University of Houston, Houston, TX; 3Dayanand Medical College and Hospital, Ludhiana, Punjab, India; 4HCA Healthcare Kingwood Hospital/University of Houston, Kingwood, TX Introduction: Candy Cane Syndrome (CCS) is an uncommon postoperative complication of Roux-en-Y gastric bypass (RYGB), a surgical intervention commonly performed to treat obesity. CCS results from a redundant blind afferent limb near the gastrojejunal anastomosis. This segment can accumulate food and secretions, resulting in postprandial pain, nausea, and vomiting. While surgical revision is the standard treatment, endoscopic approaches are emerging as minimally invasive alternatives. We present a case of successful endoscopic management of Candy Cane Syndrome, highlighting the advantages of this approach over traditional surgical methods.
Case Description/
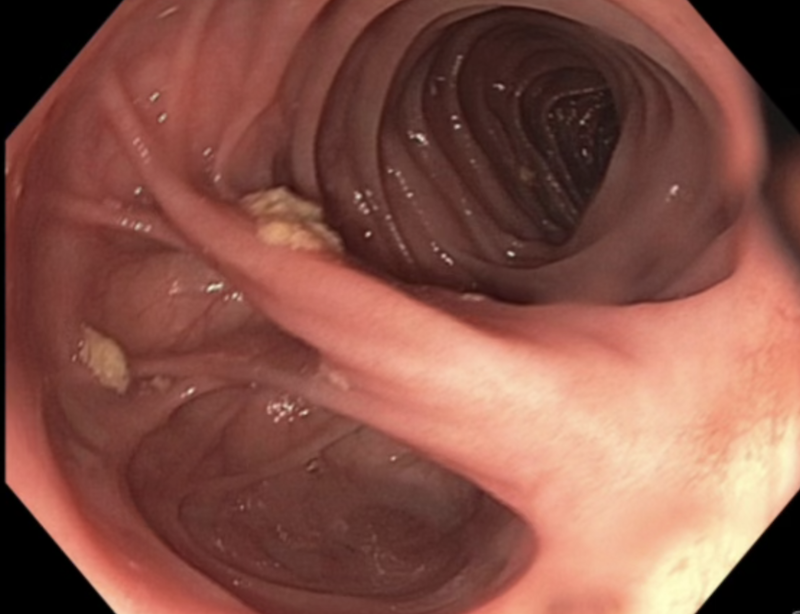
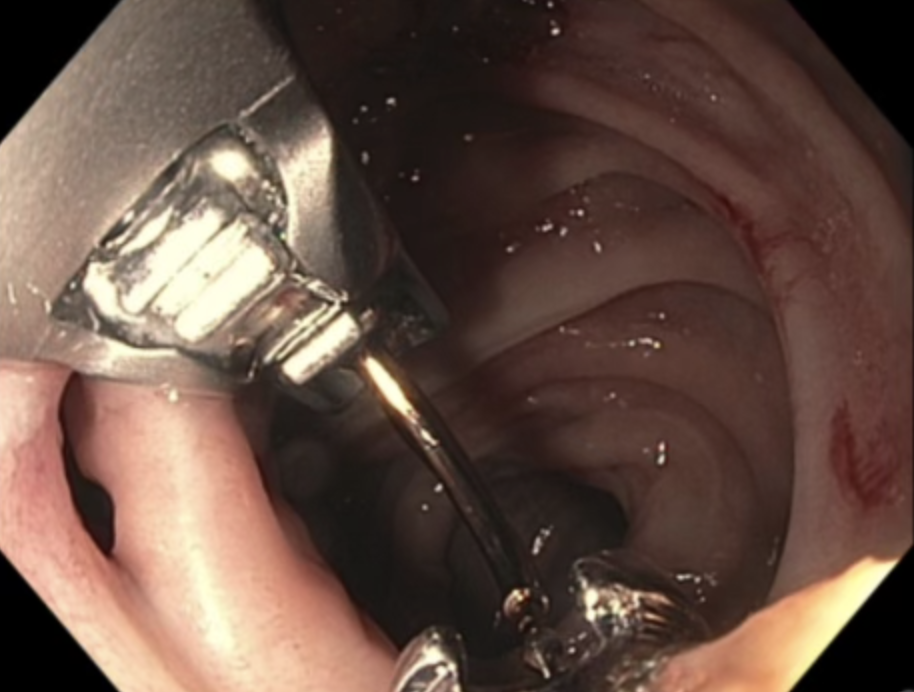
Methods: A 55-year-old African American female with a history of obesity, cholecystectomy, and prior RYGB presented with recurrent nausea, vomiting, and left upper quadrant pain radiating to the back. Gastroenterology evaluation included an initial EGD revealing a gastric pouch measuring 3 cm from the gastroesophageal junction to the gastrojejunal anastomosis, with retained food debris and mucosal congestion (Figure 1). Imaging and endoscopy confirmed the diagnosis of CCS. A repeat therapeutic EGD was performed. The OverStitch endoscopic suturing system was used to close the blind limb. The device was mounted on both ends of the endoscope and loaded with 2.0 polypropylene suture. After reinsertion, three interrupted sutures with cinches were placed, achieving excellent tissue approximation and closure of the candy cane segment (Figure 2). Minimal intra-procedural bleeding was noted, with none at the conclusion. At follow up, she reported resolution of symptoms with no further episodes of postprandial pain or vomiting. Discussion: CCS remains an under-recognized cause of post-RYGB symptoms. Although surgical revision has traditionally been the definitive treatment, endoscopic suturing offers a less invasive option, especially in patients with adhesions or co-morbidities. In this case, the OverStitch system led to successful closure of the blind limb without complications, supporting its value in both diagnosing and treating CCS. This case highlights the potential of endoscopic suturing as a minimally invasive, effective first-line therapeutic option in select post-RYGB patients. Given the favorable results, wider clinical use and further research into endoscopic approaches for CCS are warranted.
References:
Tappata M, et al., Am J Gastroenterol. 2023;118(10S):S2217. Mallangada N, et al., Am J Gastroenterol. 2023;118(10S):S1963.
Figure: Figure 1: Roux-en-Y anastomosis with large candy cane limb.
Figure: Figure 2: Endoscopic suturing performed for complete closure of candy cane limb.
Disclosures: Wafa Mehboob indicated no relevant financial relationships. Bilal Ashraf indicated no relevant financial relationships. Galvin Dhaliwal indicated no relevant financial relationships. Aakriti Soni indicated no relevant financial relationships. Ashvin Singh Dhaliwal indicated no relevant financial relationships. Sushovan Guha indicated no relevant financial relationships. Ahmed Ouni indicated no relevant financial relationships.
Wafa Mehboob, DO1, Bilal Ashraf, MD2, Galvin S. Dhaliwal, MD2, Aakriti Soni, MD2, Ashvin Singh Dhaliwal, MD3, Sushovan Guha, MD, PhD4, Ahmed Ouni, MD4. P1436 - From Pain to Relief: Minimally Invasive Endoscopic Repair of Post-Roux-en-Y Candy Cane Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.