University of Maryland School of Medicine Baltimore, MD
Cameron Amini, BS1, Farhan Ali, DO2, Abdulhameed M. Al-Sabban, MBBS3 1University of Maryland School of Medicine, Baltimore, MD; 2University of Maryland, Ijamsville, MD; 3UNIVERSITY OF MARYLAND School of Medicine, Baltimore, MD Introduction: Pyloric stenosis of the remnant stomach following Roux-en-Y gastric bypass (RNYGB) is a rare complication that can result in significant morbidity. Endoscopic therapies include are through the scope balloon dilation after accessing the remnant stomach, often requiring multiple sessions to provide therapeutic relief. We present a case of recurrent pyloric stenosis following RNYGB treated with gastrogastrostomy creation followed by a staged endoscopic ultrasound (EUS)-guided gastrojejunostomy.
Case Description/
Methods: A 74-year-old female with a history of RNYGB and recurrent pyloric stenosis treated with serial endoscopic balloon dilations presented with complaints of persistent epigastric pain with nausea and vomiting. CT of her abdomen revealed marked fluid distention of the excluded stomach and thickening of the pylorus, consistent with prior history of pyloric stenosis.
Given symptom recurrence despite previous interventions, it was decided to proceed with the creation of an EUS-guided gastrogastrostomy followed by eventual gastrojejunostomy. First, an Endoscopic Ultrasound-directed transGastric ERCP (EDGE) procedure was performed to gain access to the excluded stomach. A 20 x 10 mm lumen-apposing metal stent (LAMS) was successfully placed via endoscopic ultrasound, creating the gastrogastrostomy.
The patient was then brought back 3 weeks later for EUS-guided gastrojejunostomy. Via endoscopy a nasocystic tube was placed across the pylorus to insufflate the jejunum with a mixture of contrast and methylene blue. The echoendoscope was introduced into the excluded stomach and using a 20 mm x 10 mm LAMS a gastrojejunostomy was created. Proper positioning was confirmed using both endoscopic and fluoroscopic guidance. The patient tolerated the procedure well, without complication. Discussion: Recurrent pyloric stenosis after RNYGB is rare but can be severely debilitating due to ballooning of the excluded stomach with symptoms arising from the pressure effect in the abdomen.
EUS-guided gastrojejunostomy using LAMS offers a novel minimally invasive approach by creating a fistulous tract between the remnant stomach and jejunum, bypassing the stenotic site. This obviates the need for repeated dilations and serves as an alternative for patients who have symptoms refractory to traditional treatment options avoiding the need for surgery.
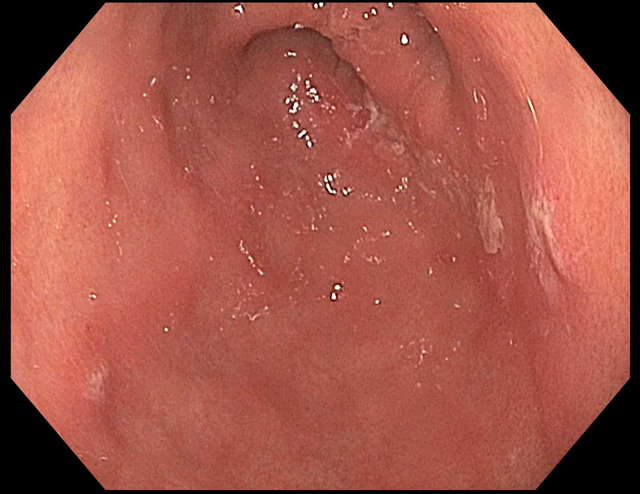
Figure: Pyloric stenosis at the remnant stomach
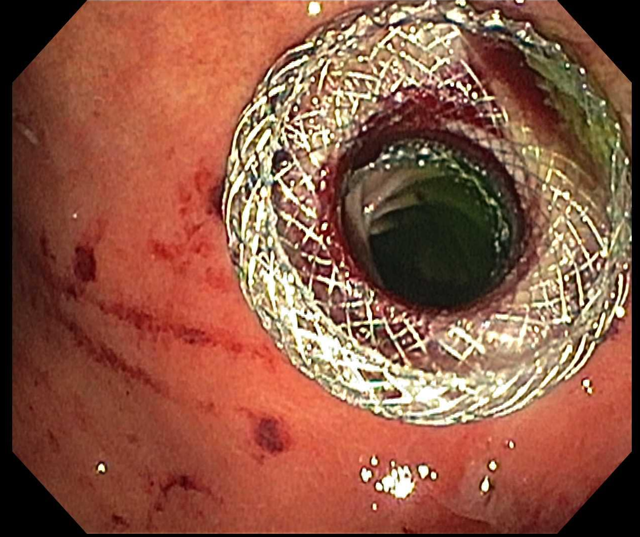
Figure: LAMS at the gastrojejunostomy across from the remnant stomach to the proximal jejunum.
Disclosures: Cameron Amini indicated no relevant financial relationships. Farhan Ali indicated no relevant financial relationships. Abdulhameed Al-Sabban indicated no relevant financial relationships.
Cameron Amini, BS1, Farhan Ali, DO2, Abdulhameed M. Al-Sabban, MBBS3. P1435 - Recurrent Pyloric Stenosis in a Roux-en-Y Gastric Bypass Patient Treated With EUS-Guided Gastrojejunostomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Cameron Amini, BS photo")