Rachel Pray, DO, Amberly Vaughan, MD, Wassem Juakiem, MD Keesler Medical Center, Biloxi, MS Introduction: Bouveret Syndrome is a rare form of gallstone ileus caused by a cholecystoduodenal fistula allowing gallstone migration into the duodenum, leading to gastric outlet obstruction. Management can be complex, often requiring advanced endoscopic techniques or surgery. Early diagnosis is critical to prevent complications.
Case Description/
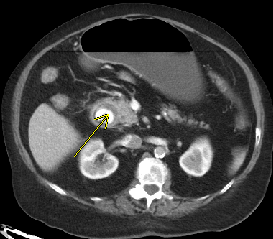
Methods: An 84-year-old female presented with one week of worsening right upper quadrant abdominal pain and persistent vomiting. She was hemodynamically stable with mild right upper quadrant tenderness and a leukocytosis of 13,600 U/L. Computed tomography (CT) imaging demonstrated acute cholecystitis, pneumobilia, a cholecystoduodenal fistula, and a large gallstone obstructing the proximal duodenum—findings consistent with Bouveret Syndrome.
She was started on antibiotics, and Gastroenterology was consulted. Endoscopy revealed a 5 cm gallstone impacted in the first portion of the duodenum. Stone removal proved highly challenging. Mechanical lithotripsy and electrohydraulic lithotripsy were attempted without success. Ultimately, holmium laser lithotripsy was used to fragment the stone, with approximately 75% of the stone removed and the remainder passed distally. The obstruction was resolved without immediate complications, and surgery was initially avoided. Follow-up imaging showed residual fragments within a large duodenal diverticulum. General Surgery recommended observation unless symptoms recurred.
Three weeks later, the patient re-presented with abdominal pain. Repeat imaging revealed distal small bowel obstruction due to gallstone impaction. She underwent laparoscopic small bowel resection with stone retrieval. The surgery was well tolerated, and she had an uneventful postoperative course. Discussion: Bouveret Syndrome most often affects elderly women with underlying gallbladder disease, although our patient had no prior history. Diagnosis is typically made by CT or esophagogastroduodenoscopy, with endoscopy being the first-line treatment. Various modalities, including mechanical and electrohydraulic lithotripsy, may be required. In this case, holmium laser lithotripsy enabled successful fragmentation of a large impacted stone, initially avoiding surgery. However, delayed distal obstruction necessitated operative intervention. Early multidisciplinary involvement is essential for optimal outcomes, particularly in refractory or complicated cases.
Figure: Gallstone present in the first part of the duodenum, visualized on CT imaging.
Figure: Attempts to extract the 5cm stone with biliary basket were partially successful.
Disclosures: Rachel Pray indicated no relevant financial relationships. Amberly Vaughan indicated no relevant financial relationships. Wassem Juakiem indicated no relevant financial relationships.
Rachel Pray, DO, Amberly Vaughan, MD, Wassem Juakiem, MD. P1431 - Gallstones on the Menu: A Rare Cause of Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")