P1416 - Safety and Efficacy of Intracholecystic Interventions Through Cholecystoduodenostomy or Cholecystogastrostomy Created During EUS-Guided Gallbladder Drainage
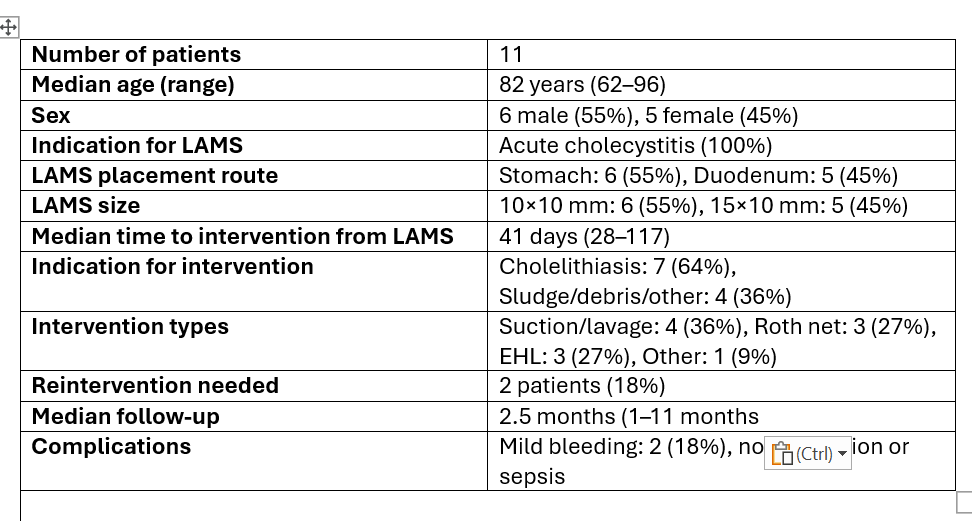
Aqsa Khan, MD1, Ganesh Aswath, MD2, Ricardo J. Torres, MD3, Harishankar Gopakumar, MD4, Neil R. Sharma, MD5 1Parkview Health Center, Fort Wayne, IN; 2SUNY Upstate Medical University, Syracuse, NY; 3University of Puerto Rico, San Juan, Puerto Rico; 4University of Illinois College of Medicine, Peoria, IL; 5Banner Health, Phoenix, AZ Introduction: Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) via cholecystoduodenostomy or cholecystogastrostomy using lumen-apposing metal stents (LAMS) has emerged as a preferred treatment for acute cholecystitis in patients unfit for surgery. While EUS-GBD is effective for gallbladder drainage, data on subsequent intracholecystic interventions performed through the internal ostomy tract remain limited. We evaluated the safety, efficacy, and outcomes of diagnostic and therapeutic intracholecystic interventions performed after EUS-GBD through cholecystoduodenostomy or cholecystogastrostomy Methods: This single-center retrospective study reviewed electronic medical records (EMR) of consecutive patients who underwent intracholecystic interventions following EUS-guided gallbladder drainage (EUS-GBD) with cholecystoduodenostomy or cholecystogastrostomy from January 2017 to April 2024. Inclusion criteria consisted of patients who had interventions performed through the internal gallbladder ostomy created by lumen-apposing metal stent (LAMS) placement. Patients who only had LAMS removal without further gallbladder intervention were excluded Results: A total of 11 patients were included (median age 82 years; range 62–96; 55% male). All underwent LAMS placement (Axios, 100%) for acute cholecystitis, with stent placement via the stomach (55%) or duodenum (45%). LAMS sizes were 10 mm × 10 mm (55%) or 15 mm × 10 mm (45%), with pigtail stents placed in 1 patient (10%). Median duration from LAMS placement to intervention was 41 days (range 28–117). Indications for intervention were cholelithiasis (64%) and sludge, debris, or other lesions (36%). The types of interventions included suction/lavage retrieval (36%), Roth net retrieval (27%), electrohydraulic lithotripsy (EHL, 27%), and other methods (stone removal with snare) (9%). Two patients (18%) required a second intervention (1 Holmium laser, 1 EHL). Median follow-up was approximately 2.5 months (range 1–11 months). Complications were limited to mild oozing bleeding in 2 patients (18%), which resolved spontaneously without intervention; no perforations or sepsis were reported Discussion: Intracholecystic interventions through EUS-GBD-created internal ostomies are safe and effective for achieving gallbladder clearance in nonsurgical patients. This minimally invasive approach may reduce the need for surgical intervention. Larger prospective studies are warranted to confirm these findings and evaluate long-term outcomes
Figure: Table 1. Patient and Procedure Characteristics
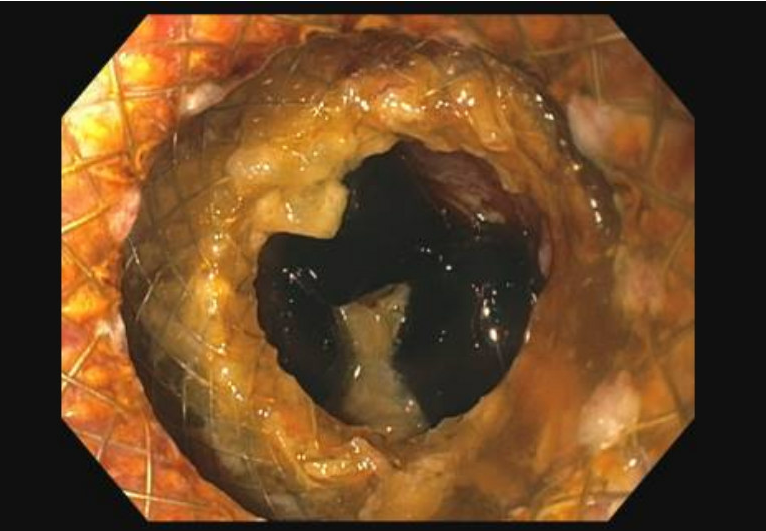
Figure: Figure 1: Endoscopic view of a lumen-apposing metal stent (LAMS) creating a cholecystoduodenostomy, with visualization of bile and gallbladder contents through the stent lumen
Disclosures: Aqsa Khan indicated no relevant financial relationships. Ganesh Aswath indicated no relevant financial relationships. Ricardo J. Torres indicated no relevant financial relationships. Harishankar Gopakumar indicated no relevant financial relationships. Neil R. Sharma: Boston Scientific – Consultant. Medtronic – Consultant. Olympus – Consultant. STERIS – Consultant.
Aqsa Khan, MD1, Ganesh Aswath, MD2, Ricardo J. Torres, MD3, Harishankar Gopakumar, MD4, Neil R. Sharma, MD5. P1416 - Safety and Efficacy of Intracholecystic Interventions Through Cholecystoduodenostomy or Cholecystogastrostomy Created During EUS-Guided Gallbladder Drainage, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")