Pinky Bai, MD1, Amro Abdellatief, MD1, Hetu Patel, MD1, Abay Gobezie, MD1, Ali Chand, MD1, Nakul Ganju, MD2, Sameer Garlapati, MD1, Angesom Kibreab, MD1 1Howard University Hospital, Washington, DC; 2Department of Medicine, Howard University Hospital, Washington, DC Introduction: Clinical manifestations of cytomegalovirus (CMV) infections vary from asymptomatic infections in healthy people to life-threatening end-organ dysfunction in immunocompromised patients. Studies have reported that acute CMV infection has been associated with venous thrombosis. We present a rare case of acute superior mesenteric vein (SMV) and portal vein thrombosis in an immunocompetent patient with acute CMV infection.
Case Description/
Methods: A 28-year-old male with medical history of obesity presented with 2 days of sharp, 9/10 LUQ pain that radiates to the back, associated with subjective fevers, nausea and loose stools. Patient denies any recent travel, sick contacts, or any other known medical conditions. He takes no medications or herbal supplements.
Patient was tachycardic to 140/minute, febrile to 102.5-degree Fahrenheit, tachypneic at 20/minute with a normal oxygen saturation on room air. Physical exam revealed LUQ tenderness to superficial and deep palpation. Labs showed leukocytosis with WBC of 18.4 x10E9 with predominant lymphocytes of 10.65 x10E9, BUN/Cr of 1.26 mg/dl, elevated transaminases with ALT 95 IU/L, AST 61 IU/L, ALK 146 g/dl with normal bilirubin. HIV, T-spot and acute hepatitis workup were negative. Blood and stool cultures, C. diff, stool ova and parasites were negative while fecal leukocytes were positive.
US duplex of lower extremity and CT-angio of chest was negative for DVT and pulmonary embolism respectively. CT-abdomen/pelvis revealed SMV and portal vein thrombosis, hepatomegaly, as well as splenomegaly with multiple splenic infarcts. Patient was started on heparin infusion. Thrombophilia workup was negative, and transthoracic echo was negative for infectious endocarditis. Viral serology testing was positive for CMV IgM and CMV PCR was elevated at 1,222 IU/ml. He was started on ganciclovir and improved clinically. And was discharged on warfarin. Discussion: A meta-analysis has shown that there were nearly 100 cases of CMV-associated thrombosis in the medical literature. A prospective study concluded that acute CMV infection might be associated with an increased short-term VTE risk. A systematic review showed that in immunocompetent patients, splanchnic vein thrombosis (SVT) and splenic infarction occur in approximately half of the published cases of CMV-associated VTE. Our case highlights that clinicians should be suspicious for acute CMV-induced thrombosis when young, immunocompetent patient present with thrombosis in unusual sites such as portal vein or SMV.
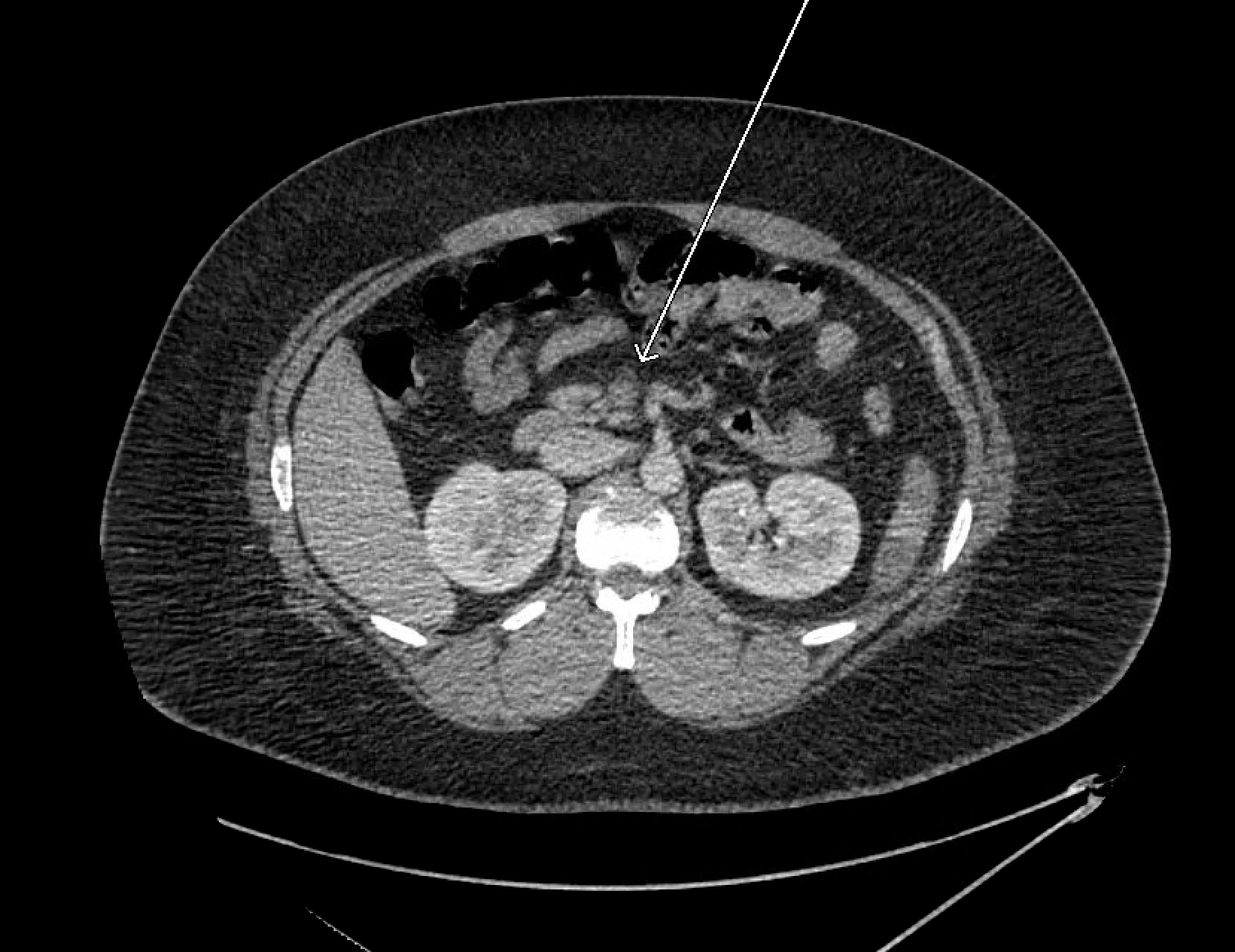
Figure: Axial CT image reveals a filling defect within the splenic vein (arrow), consistent with splenic vein thrombosis.
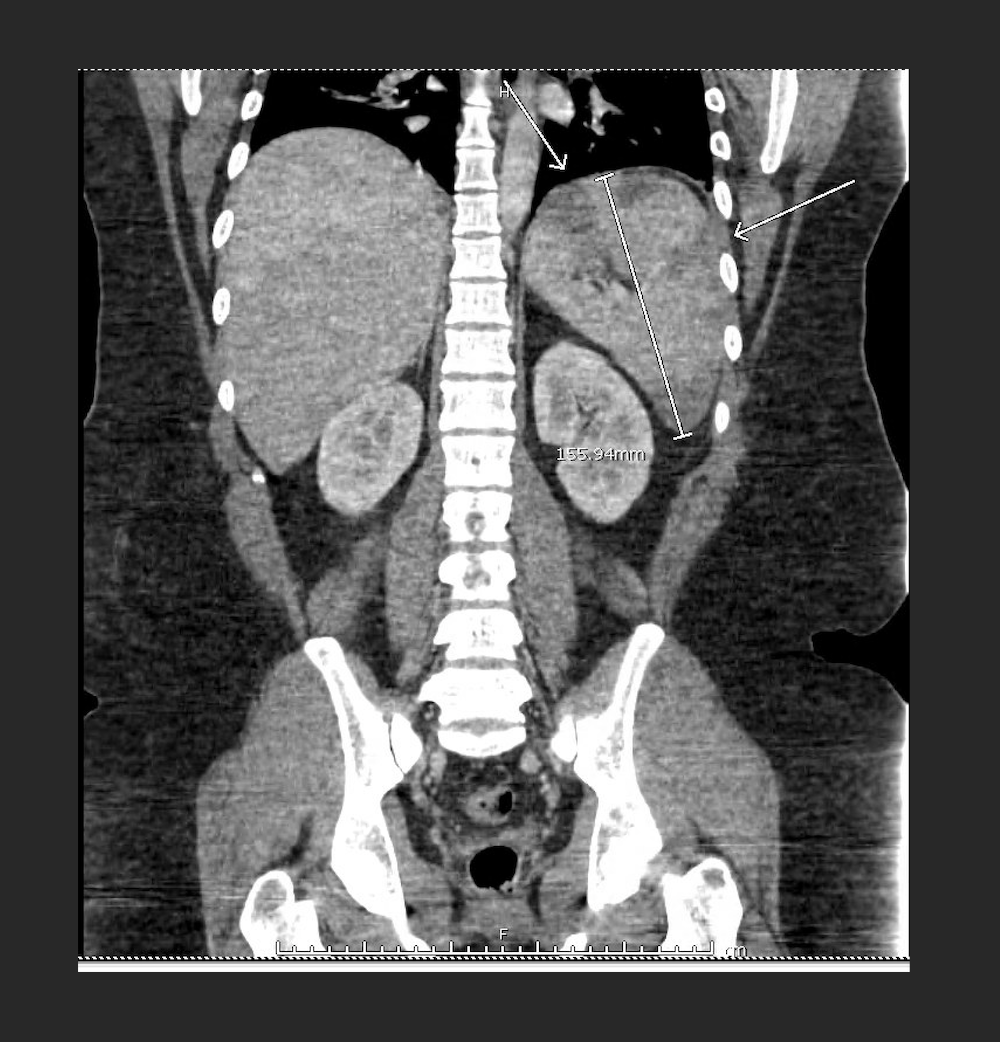
Figure: Coronal CT image shows a significantly enlarged spleen (white arrow) with multiple splenic infarcts.
Disclosures: Pinky Bai indicated no relevant financial relationships. Amro Abdellatief indicated no relevant financial relationships. Hetu Patel indicated no relevant financial relationships. Abay Gobezie indicated no relevant financial relationships. Ali Chand indicated no relevant financial relationships. Nakul Ganju indicated no relevant financial relationships. Sameer Garlapati indicated no relevant financial relationships. Angesom Kibreab indicated no relevant financial relationships.
Pinky Bai, MD1, Amro Abdellatief, MD1, Hetu Patel, MD1, Abay Gobezie, MD1, Ali Chand, MD1, Nakul Ganju, MD2, Sameer Garlapati, MD1, Angesom Kibreab, MD1. P1339 - Acute CMV Infection Presenting as Superior Mesenteric Vein and Portal Vein Thrombosis: A Rare Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.