Dayanand Medical College and Hospital Rancho Cucamonga, CA
Bhavik Sethi, MBBS1, Rajat Bansal, MBBS, MD, DM1, Hitendra Garg, MBBS, MD, DM1, Abhishek Rajput, MBBS1, Srishti Ahluwalia, MBBS2, Raghav Chanday, MBBS3, Saumya Ahluwalia, MBBS2 1Apollo Hospital, New Delhi, Delhi, India; 2Dayanand Medical College and Hospital, Rancho Cucamonga, CA; 3Dayanand Medical College and Hospital, Ludhiana, Punjab, India Introduction: Hepatitis A virus (HAV) is a RNA virus transmitted primarily via fecal-oral route. While the majority of HAV infections are self-limiting and resolve without significant complications, severe cases may occasionally result in acute liver failure (ALF), particularly in older adults or those with underlying liver disease.
Pancreatitis is a rare extra-hepatic manifestation of HAV infection. Although mild elevations of pancreatic enzymes may occur during acute viral hepatitis, clinically significant acute pancreatitis, especially acute necrotizing pancreatitis (ANP) is extremely uncommon.
We are presenting a case of a young male diagnosed with both ANP and ALF secondary to acute HAV infection.
Case Description/
Methods: A 17-year-old male presented with fever for seven days followed by jaundice, severe epigastric pain, vomiting for 3 days and altered mental status for one day.
Investigations revealed elevated liver enzymes (AST 3300 IU/L; ALT 9374 IU/L), hyperbilirubinemia (Total bilirubin 3.9 mg/dL; Direct bilirubin 2.5 mg/dL), coagulopathy (INR-1.6) and raised ammonia level (312μmol/L). HAV IgM antibodies were positive. Serum lipase (1540 IU/L) and amylase (1789 IU/L) were markedly elevated, suggesting acute pancreatitis.
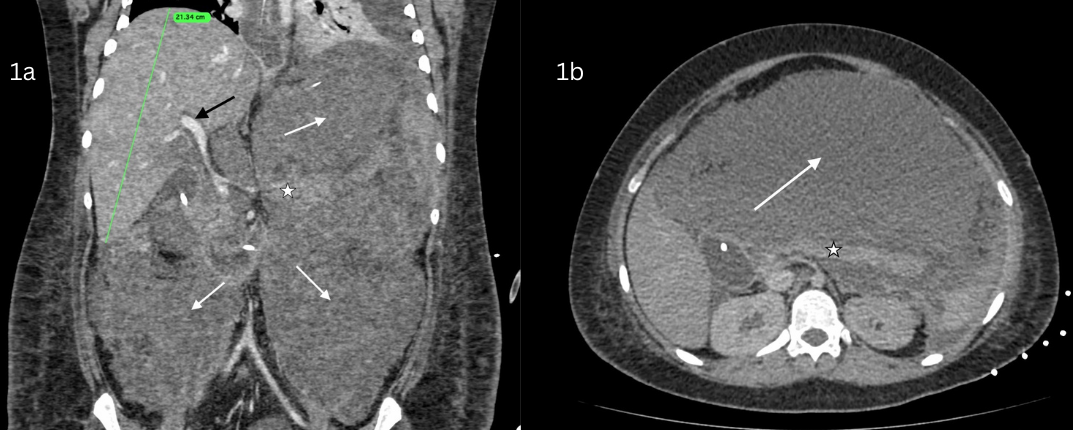
Contrast-enhanced computed tomography (CECT) abdomen showed hepatomegaly without biliary obstruction and diffuse pancreatic inflammation with peripancreatic collection (Figure 1).
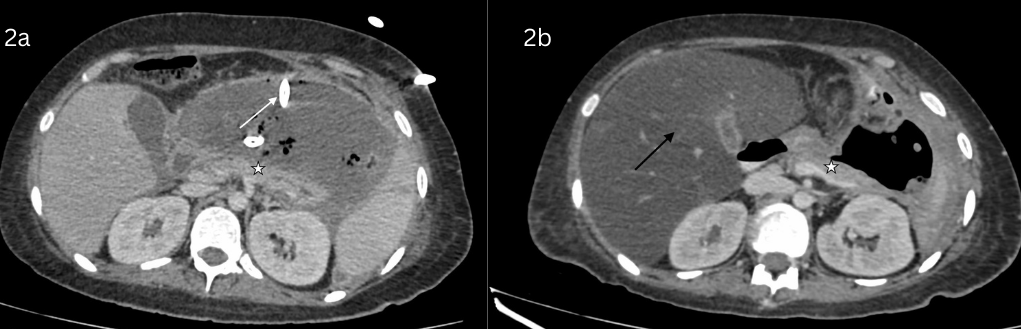
Due to worsening encephalopathy and respiratory failure he was intubated and managed in the ICU with continuous renal replacement and supportive therapy. Due to worsening sepsis, percutaneous drainage of peripancreatic collection was done (Figure 2). He later underwent retroperitoneal debridement and necrosectomy for infected peripancreatic collections. The patient gradually improved and was discharged in stable condition. Discussion: ALF occurs in less than 1% HAV cases. Combination of ANP and ALF due to HAV is very rare ( < 0.1% cases) and the overlapping symptoms can make diagnosis and management intricately challenging.
HAV is postulated to cause ALF from an overwhelming immune-mediated response leading to massive hepatocyte necrosis and pancreatitis due to direct viral; immune mediated injury to pancreatic tissue and ampullary oedema causing pancreatic fluid outflow obstruction.
This case highlights the importance of considering extra-hepatic complications in viral hepatitis, especially in severe cases and the role of early diagnosis and intensive supportive measures for a favourable outcome.
Figure: Figure 1. Coronal (1a) and Axial (1b) CECT abdomen in porto-venous phase showing hepatomegaly (liver span-21.34 cm) with periportal edema (black arrow) suggesting acute hepatitis along with edematous pancreas (star) with large peripancreatic collection (white arrows) suggesting acute necrotizing pancreatitis.
Figure: Figure 2. Axial CECT abdomen after 1 month (2a) showing peripherally enhancing organized peripancreatic collection (white arrow) which has regressed in size with drainage tube in situ with air foci. Follow up CECT abdomen after 4 months (2b) shows resolution of collection with diffuse fatty changes in liver (black arrow) and atrophic changes in pancreas (star).
Disclosures: Bhavik Sethi indicated no relevant financial relationships. Rajat Bansal indicated no relevant financial relationships. Hitendra Garg indicated no relevant financial relationships. Abhishek Rajput indicated no relevant financial relationships. Srishti Ahluwalia indicated no relevant financial relationships. Raghav Chanday indicated no relevant financial relationships. Saumya Ahluwalia indicated no relevant financial relationships.
Bhavik Sethi, MBBS1, Rajat Bansal, MBBS, MD, DM1, Hitendra Garg, MBBS, MD, DM1, Abhishek Rajput, MBBS1, Srishti Ahluwalia, MBBS2, Raghav Chanday, MBBS3, Saumya Ahluwalia, MBBS2. P1334 - Rare Presentation of a Common Virus: Severe Acute Necrotizing Pancreatitis Secondary to Hepatitis A Infection With Acute Liver Failure, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.