Hospital Roosevelt / Gastri-k Guatemala City, San Marcos, Guatemala
Ninoska Meléndez, 1, Jorge Pacheco, 1, Abel Sanchez, MD, MSc2 11. Gastroenterology and Endoscopy Unit, Hospital Roosevelt Guatemala, Guatemala City, Quetzaltenango, Guatemala; 2Hospital Roosevelt / Gastri-k, Guatemala City, San Marcos, Guatemala Introduction: Colorectal cancer (CRC) is a serious complication in patients with Crohn's disease (CD). We present the first case of a pregnant patient in whom a routine prenatal study led to the diagnosis of colorectal adenocarcinoma and concomitant Crohn's disease
Case Description/
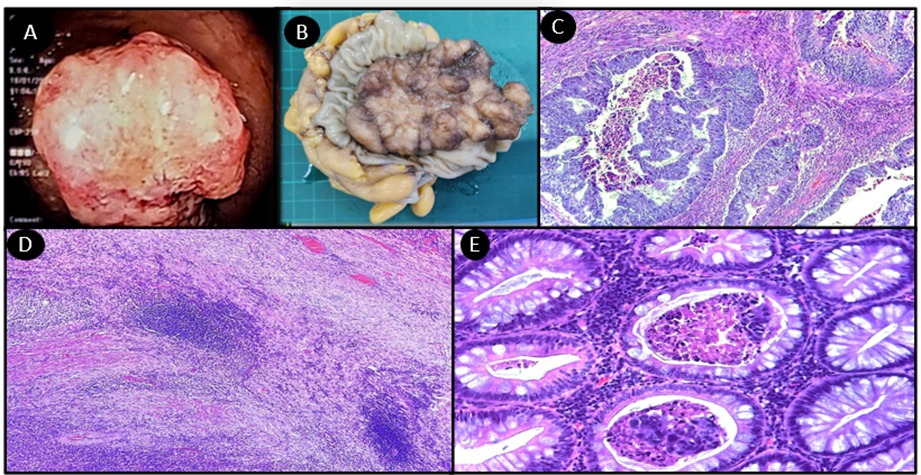
Methods: A 30-year-old Guatemalan woman presented with an eight-month history of intermittent diarrhea accompanied by blood and mucus, with approximately two daily episodes of 150 ml, associated with non-quantified fever. Two months later, while asymptomatic, during her first prenatal check-up at 12 weeks of gestation, an obstetric ultrasound revealed a mass in the sigmoid colon. A rectosigmoidoscopy was performed, identifying an intraluminal mass 20 cm from the anal margin (Figure 1A). Histopathology confirmed moderately differentiated and invasive ulcerated adenocarcinoma (Figure 1C). An exploratory laparotomy was carried out with resection of a 12 x 12 cm obstructive ulcerated polypoid mass, confirming the previous diagnosis of neoplasia (Figure 1B). Additionally, further findings compatible with Crohn's disease were found (Figure 1D, 1E). Throughout the pregnancy, the patient remained asymptomatic, with fecal calprotectin levels at 83 µg/g, C-reactive protein at 0.32 mg/dl, and an erythrocyte sedimentation rate of 28 mm/hr. The Crohn's Disease Activity Index (CDAI) was -128 points, indicating remission, with no need to initiate steroids or biological therapy during the pregnancy. At 24 weeks of gestation, chemotherapy with oxaliplatin and capecitabine was initiated, and a cesarean section was performed at 35 weeks of gestation without complications. Currently, the patient is in remission from adenocarcinoma and under surveillance. Discussion: Although the risk of colorectal cancer (CRC) is known in ulcerative colitis, there is little data on Crohn's disease (CD). Inflammatory bowel disease (IBD) increases the risk of CRC, with a worse prognosis and higher mortality. CRC in IBD appears at younger ages. Pregnancy can increase the risk of complications in CD, especially if the disease is active at conception. Remission before conception is recommended. According to other theories, during pregnancy, estrogen and progesterone strengthen the intestinal barrier, reducing IBD activity. Managing a pregnant patient with both conditions is a challenge that requires a multidisciplinary approach
Figure: FIGURE 1. A. Rectosigmoidoscopy, identifying an intraluminal mass 20 cm from the anal margin. B. Surgical specimen, mass in the sigmoid colon measuring 10x9x4 cm, weighing 155 grams. C. Upon examination at a higher magnification of 40x, a glandular neoplasm is observed, consistent with a moderately differentiated adenocarcinoma infiltrating the stroma. D. Extensive subserosal lymphoplasmacytic infiltrate is observed, with lymphoid aggregates indicative of transmural inflammation. E. Colon glands slightly increased in size, with acute inflammatory infiltrate in the crypts, active colitis, and microabscess formation, highly suggestive of Crohn's disease
Disclosures: Ninoska Meléndez indicated no relevant financial relationships. Jorge Pacheco indicated no relevant financial relationships. Abel Sanchez indicated no relevant financial relationships.
Ninoska Meléndez, 1, Jorge Pacheco, 1, Abel Sanchez, MD, MSc2. P1221 - Colorectal Cancer as Initial Presentation of Crohn's Disease in a Pregnant Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")