NewYork-Presbyterian / Weill Cornell Medical Center New York, NY
Fredella Lee, MD1, Daniel Paik, MD1, Qu Deng, MD, PhD1, David Wan, MD2 1NewYork-Presbyterian / Weill Cornell Medical Center, New York, NY; 2NewYork-Presbyterian Hospital/Weill Cornell Medical Center, New York, NY Introduction: Lymphocytic gastritis (LG) is a histological diagnosis, defined by the presence of more than 25 intraepithelial lymphocytes per 100 epithelial cells. This pattern of gastric mucosal inflammation is uncommon, occurring in < 0.3% of the general population. LG is often associated with Helicobacter pylori infection or celiac disease but can be idiopathic, with a nonspecific abdominal complaint. We present a rare case of acute upper gastrointestinal bleed (UGIB) secondary to hyperplastic polyps in a setting of LG.
Case Description/
Methods: A 67-year-old female with end stage renal disease, type 2 diabetes, coronary artery disease, nonocclusive right upper extremity deep vein thrombosis, on apixaban, and newly diagnosed stage 4 uterine carcinoma with transfusion-dependent anemia from chronic vaginal bleeding, presented for hematemesis and melena. Besides her last dose of apixaban overnight, she denied use of NSAIDs, aspirin, steroids, radiation, and or chemotherapy. In the ED, her vitals were unremarkable. Labs revealed downtrending hemoglobin (Hgb) from a baseline 10.1 g/dL four days ago to 7.1 g/dL. An initial esophagogastroduodenoscopy (EGD) was completed the next day. It showed 15 polyps ranging from 5 to 15mm, without an active bleed, but with adherent clots in the entire stomach suggestive of recent bleed. With recent anticoagulation (AC), bleeding, and difficult location of some polyps in the gastric cardia, polypectomies were deferred in favor of hemostatic clips and spray. Despite holding AC, her melena persisted and she underwent two more EGDs, days later, for hot snare removal of the remaining polyps with subsequent use of hemostatic clips and Purastat gel for post-polypectomy bleed. Prior to discharge, patient tolerated full dose AC without any recurrence of melena or drops in Hgb. Pathology reports of the initial EGDs showed hyperplastic polyps and only subsequent histologic evaluation revealed a background of lymphocytic gastritis. Discussion: Iron deficiency anemia is an uncommon but known complication of gastric hyperplastic polyps (HP); acute UGIB is even more rare. This case highlights the potential for spontaneous UGIB from HP and the role of hot snare polypectomy to achieve hemostasis. It also underscores the value of obtaining multiple biopsies in various gastric sites for optimal diagnostic accuracy. Only later histologic analyses of resected polyps showed LG. This underlying inflammatory process may explain the development of HG and guide future diagnostic testing at follow-up.
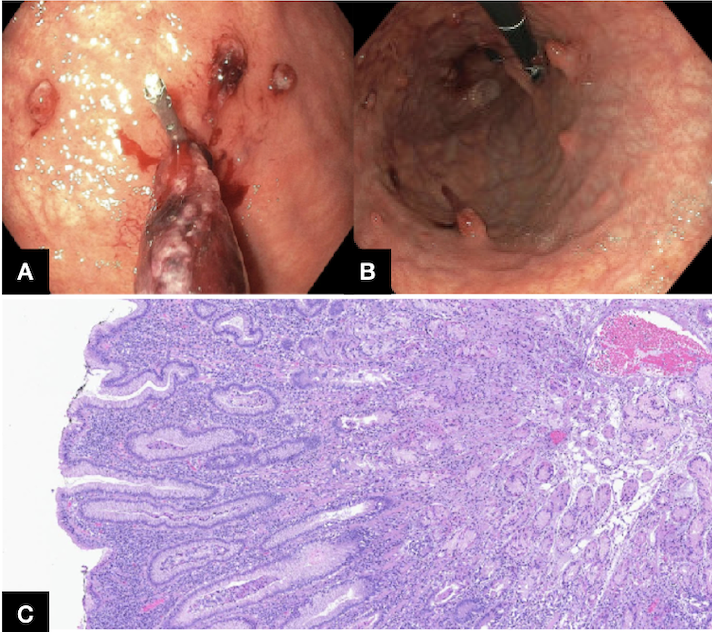
Figure: Figure A shows clip placement at the base of a large gastric polyp with an adherent clot. Figure B shows multiple gastric polyps in the gastric body. Figure C shows the background histological features of lymphocytic gastritis from biopsies of several gastric polyps.
Disclosures: Fredella Lee indicated no relevant financial relationships. Daniel Paik indicated no relevant financial relationships. Qu Deng indicated no relevant financial relationships. David Wan: Medtronic – Data Monitoring Committee.
Fredella Lee, MD1, Daniel Paik, MD1, Qu Deng, MD, PhD1, David Wan, MD2. P1009 - Bleeding Gastric Hyperplastic Polyps in the Setting of Lymphocytic Gastritis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")