University of South Florida Morsani College of Medicine Tampa, FL
Matthew Heckroth, MD, Pushpak Taunk, MD University of South Florida Morsani College of Medicine, Tampa, FL Introduction: Gastrointestinal (GI) bleeding in patients with acquired immunodeficiency syndrome (AIDS) is rare, but potentially life threatening. It may result from conditions associated with AIDS including opportunistic infection, malignancy, HIV-associated enteropathy or unrelated etiologies. We present a rare and complex case of a patient with newly diagnosed AIDS who developed hemorrhagic shock secondary to a GI bleed and was subsequently found to have diffuse large B-cell lymphoma (DLBCL) of the stomach with concomitant small bowel tuberculosis (TB).
Case Description/
Methods: A 36-year-old male with no prior medical history presented with altered mental status after being found unresponsive. He was febrile to 101 F. Labs revealed a positive HIV antibody and CD4 count of 25 cells/mm3. Workup including neuroimaging and cerebrospinal fluid analysis revealed TB meningitis and chest radiography demonstrated a miliary pattern concerning for disseminated TB.
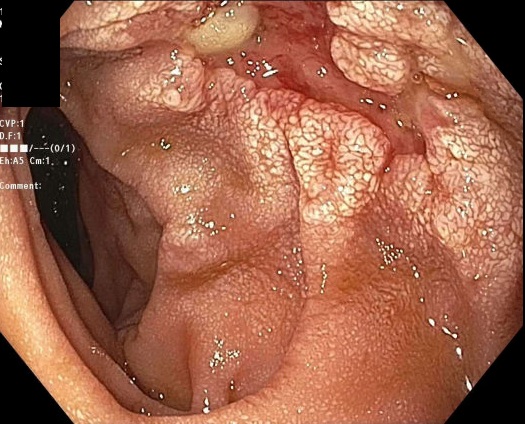
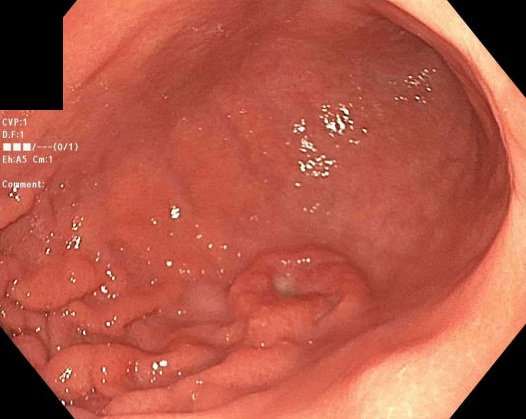
Two days into hospitalization, he developed hypotension and melena. Hemoglobin acutely dropped from 8.1 to 4.7 g/dL. Following resuscitation, he underwent esophagogastroduodenoscopy (EGD) which revealed a 2 cm ulcerated mass in the gastric body and irregular, polypoid mucosa with ulceration involving the duodenal bulb and second portion of the duodenum, but no active bleeding. Histopathology from the gastric mass confirmed DLBCL, while duodenal biopsies were positive for Mycobacterium tuberculosis. Hematology and infectious disease services were consulted, and the patient was started on DA-R-EPOCH chemotherapy for DLBCL and RIPE therapy for disseminated TB. Discussion: This case highlights the rare co-occurrence of GI DLBCL and intestinal TB presenting with GI bleeding in the setting of newly diagnosed AIDS. While both conditions are known complications of HIV/AIDS, their simultaneous involvement of the upper GI tract has not been reported. HIV-associated lymphomas often involve extra-nodal sites such as the GI tract and may present with bleeding. GI TB is most commonly localized to the ileocecal region, with duodenal involvement reported in less than 5% of cases. Endoscopically it may mimic malignancy.
The overlapping presentations of these entities pose diagnostic challenges, particularly in immunocompromised hosts. Early endoscopic evaluation with biopsy is crucial for timely diagnosis. This case highlights the need to consider both infectious and malignant causes in AIDS patients with GI bleeding and the importance of multidisciplinary management.
Figure: Duodenal Tuberculosis
Figure: Gastric lymphoma
Disclosures: Matthew Heckroth indicated no relevant financial relationships. Pushpak Taunk: Boston Scientific – Consultant. Endo Therapeutics – Consultant. Neptune Medical – Consultant.
Matthew Heckroth, MD, Pushpak Taunk, MD. P1008 - GI Bleeding in AIDS: A Rare Case of Coexisting Gastric Lymphoma and Duodenal Tuberculosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.