Weill Cornell College of Cornell University New York, NY
David Li, BS1, David Wan, MD2, Sybil L.. Olmo, FNP3, Preston Atteberry, MD2 1Weill Cornell College of Cornell University, New York, NY; 2NewYork-Presbyterian Hospital/Weill Cornell Medical Center, New York, NY; 3New York Presbyterian, Weill Cornell Medical Center, New York, NY Introduction: Renal angiomyolipomas (AMLs) are benign renal tumors composed of smooth muscle cells, adipocytes, and epithelioid cells. Renal AML is associated with tuberous sclerosis complex (TSC) and is more common in women. It is often asymptomatic but can present with abdominal or flank pain, hematuria, or spontaneous retroperitoneal hemorrhage. Despite advances in imaging, clinical recognition and management strategies for renal AMLs remain areas of ongoing research.
Case Description/
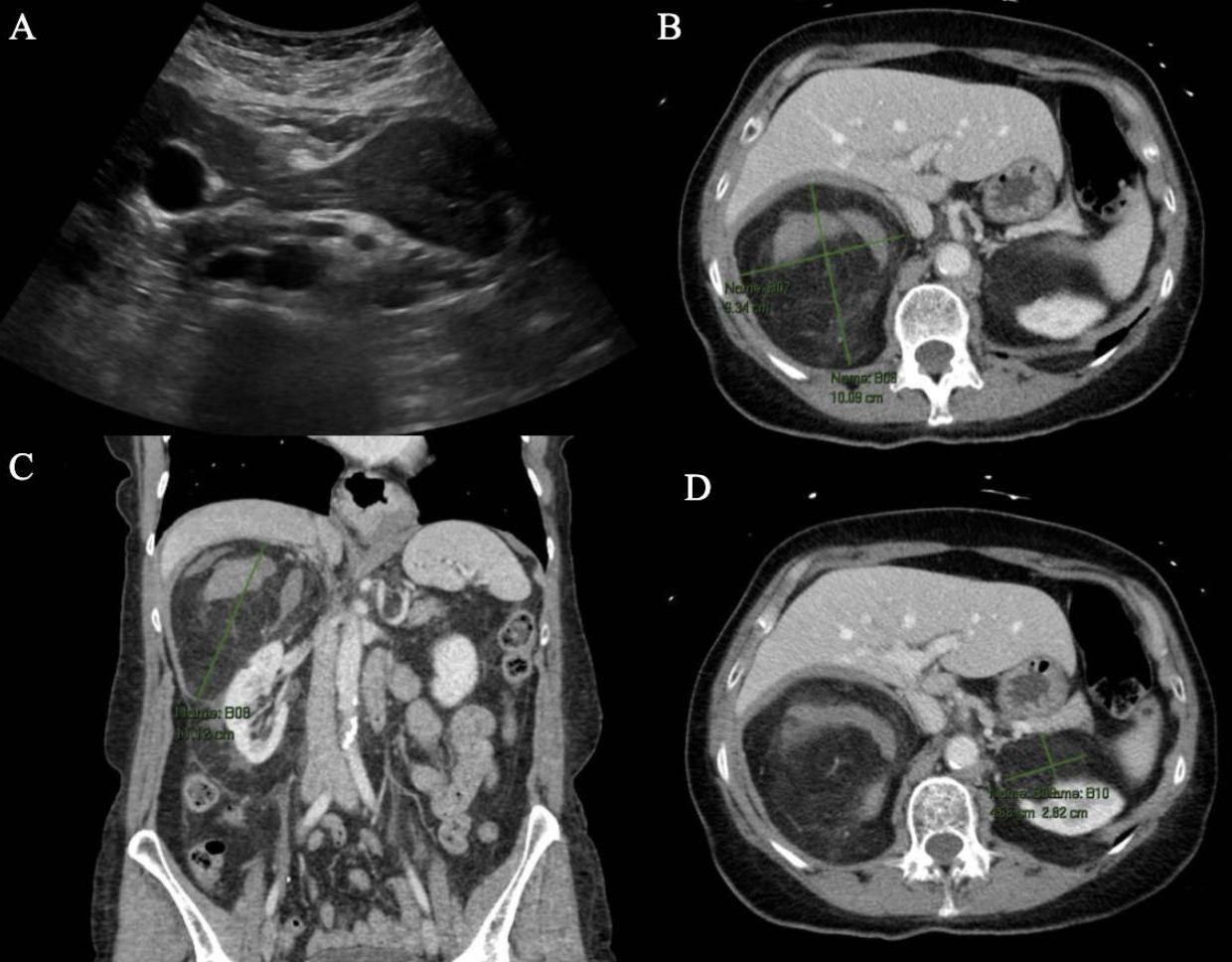
Methods: A 60-year-old woman with type 1 diabetes mellitus, Hashimoto’s thyroiditis, collagenous colitis, and bilateral renal angiomyolipomas presented to the hospital with right upper quadrant (RUQ) abdominal and right flank pain for 2 days. She also reported a fever of 38.3 C, nausea, and vomiting. Her labs were notable for WBC 12.16k/uL and absolute neutrophil count of 9.8k/uL. Abdominal ultrasound (US) revealed increased size of right AML measuring 15.0 x 10.1 x 13.9 cm, previously 9.0 x 7.7 cm, and left AML similarly showed increased size of 5.6 x 5.6 x 4.4 cm, previously 4.5 x 3.6 cm. Given the acute onset of abdominal pain, a CT abdomen and pelvis was performed, which demonstrated an 11.1 cm right AML and 5.9 cm left AML with a small new volume of hemorrhage within and surrounding the right AML without evidence of active hemorrhage (Figure 1). Given her clinical stability, no acute intervention was initiated, and she was discharged for outpatient interventional radiology (IR) management. Based on the increased size of the right AML ( > 4 cm), IR performed image-guided right main renal artery embolization without any complications. Discussion: Renal AMLs are usually benign and asymptomatic, requiring no intervention. Surveillance is appropriate for small, asymptomatic lesions, while larger or symptomatic AMLs may require intervention. Artery embolization, ablation, or surgical resection are effective options. In this patient with hemorrhage from the right AML, outpatient IR-guided embolization was performed
successfully, stabilizing the lesion and preventing further morbidity. She initially presented with RUQ and flank pain, which overlaps with other diagnoses such as cholecystitis, nephrolithiasis, or pyelonephritis. It is essential to recognize signs of hemorrhage, such as abdominal or flank pain, hematuria, hypertension, anemia, and impaired kidney function, for patients with renal AML to diagnose in a timely fashion and provide appropriate treatment.
Figure: Figure 1: A. Abdominal ultrasound (US) trans pancreas of the right kidney; B. CT AP axial view of right renal AML; C. Coronal view of right renal AML; D. Axial view of left renal AML
Disclosures: David Li indicated no relevant financial relationships. David Wan: Medtronic – Data Monitoring Committee. Sybil Olmo indicated no relevant financial relationships. Preston Atteberry indicated no relevant financial relationships.
David Li, BS1, David Wan, MD2, Sybil L.. Olmo, FNP3, Preston Atteberry, MD2. P1002 - A Case of Bleeding Renal Angiomyolipoma Presenting as Right Upper Quadrant (RUQ) Abdominal Pain, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")