St. Luke's University Health Network Bethlehem, PA
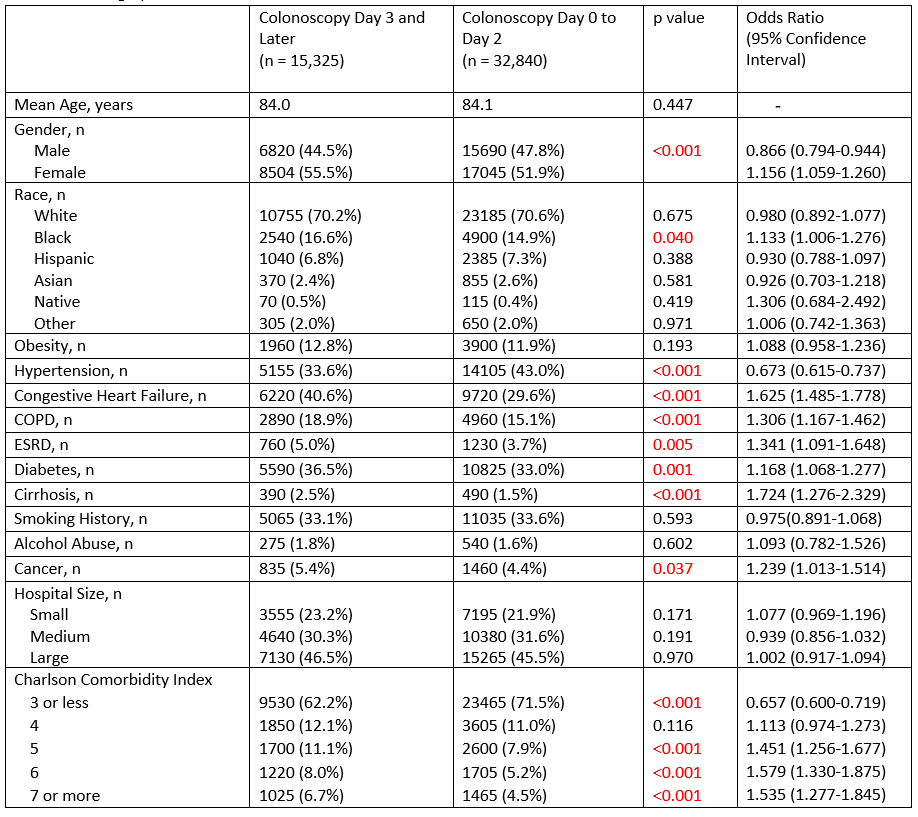
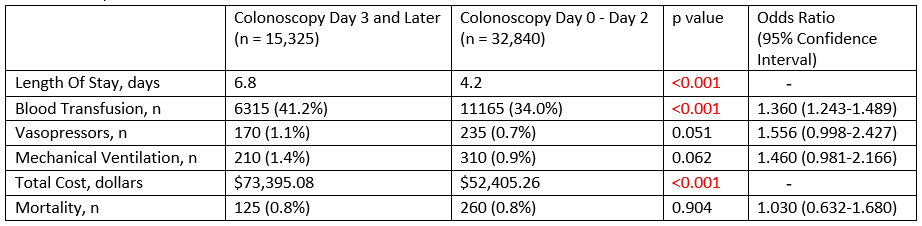
Het Patel, DO, Hammad Liaquat, MD St. Luke's University Health Network, Bethlehem, PA Introduction: Octogenarians with lower gastrointestinal bleeding represent a growing and vulnerable population. While colonoscopy is a key diagnostic and therapeutic tool, the optimal timing remains uncertain. The goal of this study is to compare the risks and outcomes associated with early versus late colonoscopy in elderly patients presenting with lower GI bleed. Methods: This is a retrospective cohort study using National Inpatient Sample data including patients hospitalized between 2019 and 2022 age 80 to 89 who presented with a lower GI bleed and underwent colonoscopy. The study compares risk factors including demographics and chronic medical conditions along with hospitalization complications between patients who underwent late colonoscopy (Day 3 and onward) and early colonoscopy (Day 0-2). Statistical analyses were all performed using STATA software. Results: Of the 46,165 patients who met our inclusion criteria, a majority (55.3%) were female with average age around 84 in both groups. We found that in this demographic, females (OR 1.156 95% CI 1.059-1.260), African Americans (OR 1.133; 95% CI 1.006-1.276), and patients with CHF (OR 1.625; 95% CI 1.485-1.778), COPD (OR 1.306; 95% CI 1.167-1.462), ESRD (OR 1.341; 95% CI 1.091-1.648), diabetes (OR 1.168; 95%CI 1.068-1.277), cirrhosis (OR 1.724 95% CI 1.276-2.329), cancer (OR 1.239; 95% CI 1.013-1.514) and Charlson Comorbidity Index (CCI) >5 were statistically significantly (p< 0.05) less likely to undergo early colonoscopy. On the other hand, males (OR 0.866; 95% CI 0.794-0.944), patients with hypertension (OR 0.673; 95% CI 0.615-0.737), and CCI ≤ 3 were significantly (p< 0.05) more likely to undergo early colonoscopy. Hospital size did not impact time to colonoscopy in these patients (p≥ 0.05). Additionally, patients with later colonoscopy had a significantly greater (p< 0.05) length of stay (LOS), cost of stay, and required blood transfusions (Table 2). There was no difference in vasopressor requirement, mechanical ventilation, and mortality between the late and early colonoscopy groups (p≥ 0.05). Discussion: Our study showed that patients in their 80s with greater comorbidities were more likely to have delayed colonoscopy and while this affected LOS, it did not impact the risk of mortality. Additionally, we found females and African Americans were more likely to have delayed endoscopy which may represent an underlying healthcare disparity. Further studies are necessary to identify what objective parameters influenced the timing of colonoscopy.
Figure: Table 1: Demographics and Comorbidities
Figure: Table 2: Hospitalization Outcomes
Disclosures: Het Patel indicated no relevant financial relationships. Hammad Liaquat indicated no relevant financial relationships.
Het Patel, DO, Hammad Liaquat, MD. P0942 - Eighty and Bleeding: Comparative Risk of Early vs Late Colonoscopy in Octogenarians With Lower GI Bleeds, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Het Patel, DO photo")