HCA Houston Healthcare/University of Houston College of Medicine Houston, TX
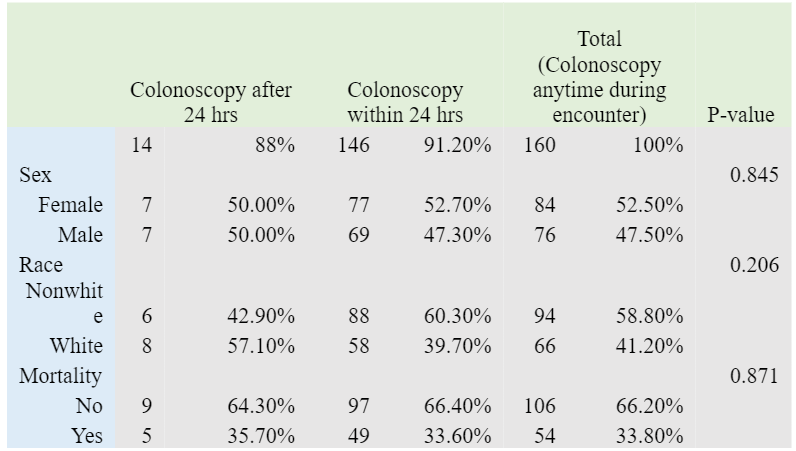
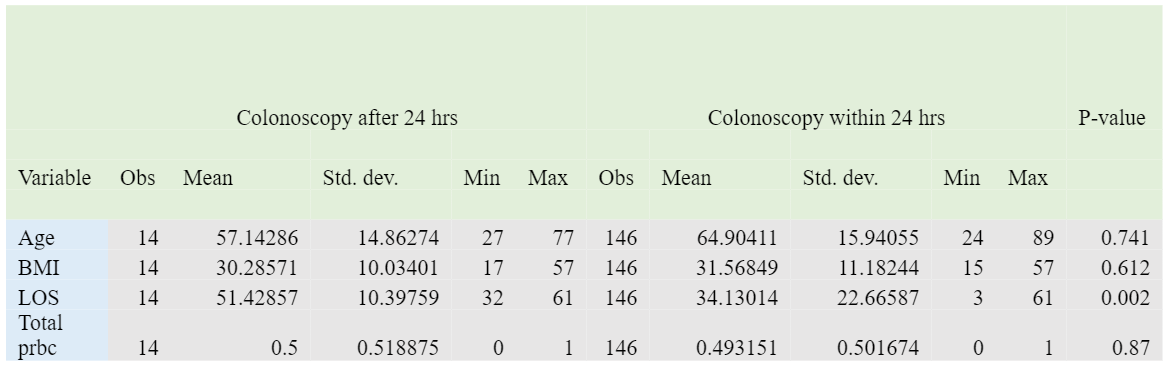
Ammar Hasan, MD1, Galvin S. Dhaliwal, MD2, Saad Farooqi, MD3, Sushovan Guha, MD, PhD4 1HCA Houston Healthcare/University of Houston College of Medicine, Houston, TX; 2HCA Healthcare Kingwood Hospital/University of Houston, Houston, TX; 3Insight Hospital & Medical Center, Houston, TX; 4Houston Regional Gastroenterology Institute and University of Houston, Sugar Land, TX Introduction: Managing acute lower GI bleeding in hemodynamically unstable patients can be challenging. Colonoscopy is the recommended diagnostic and therapeutic procedure of choice after achieving stabilization. Although early colonoscopy within 24 hours is preferred but there are no set guidelines about the timing of colonoscopy. Methods: We conducted a retrospective review of adult patients (age ≥18) admitted between January 2018 and January 2023 across a large hospital system with acute lower GI bleeding with hemodynamic instability, along with active extravasation noted on CTA abdomen. We compared inpatient mortality as the primary outcome between patients who underwent colonoscopy within 24 hours versus those who received it after 24 hours (Table 1). Secondary outcomes included ICU length of stay and blood transfusion requirements (Table 2). Standard statistical methods were used to compare outcomes between the two groups. Results: Of the 160 patients who underwent colonoscopy during hospitalization, 146 patients received the procedure within 24 hours. The mean age of the cohort was 65 years. There was no statistically significant difference in inpatient mortality between the early and late colonoscopy groups (33.6% vs. 35.7%, p=0.871). Similarly, both groups required comparable amounts of blood transfusion (mean 0.49 vs. 0.50 units, p=0.87). Patients who underwent colonoscopy within 24 hours had a statistically significant reduction in ICU length of stay compared to those who did not (p=0.002). Discussion: In this study of hemodynamically unstable patients with acute lower GI bleeding, the timing of colonoscopy within the first 24 hours did not significantly impact mortality or transfusion needs. These findings suggest that early colonoscopy is safe but may not provide a survival or hemostatic advantage over delayed procedures in this population. However, early intervention may still play a role in diagnosis, care coordination, and resource utilization, even if traditional outcomes, including mortality, are unaffected. Given the lack of formal guidelines on optimal timing, these results contribute to ongoing discussions about balancing clinical urgency with patient stability and procedural readiness. Prospective studies are needed to define which subgroups, if any, may benefit most from early colonoscopy.
Figure: Table 1
Figure: Table 2
Disclosures: Ammar Hasan indicated no relevant financial relationships. Galvin Dhaliwal indicated no relevant financial relationships. Saad Farooqi indicated no relevant financial relationships. Sushovan Guha indicated no relevant financial relationships.
Ammar Hasan, MD1, Galvin S. Dhaliwal, MD2, Saad Farooqi, MD3, Sushovan Guha, MD, PhD4. P0920 - Early vs Delayed Colonoscopy in Hemodynamically Unstable Acute Lower GI Bleed: A Retrospective Comparison of Clinical Outcomes, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.