CHI Health Creighton University Medical Center Omaha, NE
Casey M. DeBeltz, DO, Clive J. Miranda, DO, MSc, Aditya Avula, DO, Shane Manatsathit, MD CHI Health Creighton University Medical Center, Omaha, NE Introduction: Marginal ulcers and gastrojejunal anastomotic strictures are common complications after gastric bypass surgery. We present a case of rapid improvement in a refractory anastomotic ulcer with stricture after 4 week treatment with a PCAB.
Case Description/
Methods: A 52-year-old male with a history of longstanding GERD was initially seen by the GI service for development of melena during an unrelated hospitalization for cauda equina syndrome. EGD at the time was significant for multiple duodenal ulcers and LA grade D esophagitis. Prior to follow up EGD, he suffered from a D2/D3 duodenal ulcer perforation leading to Cellan-Jones patch reconstruction with pyloric exclusion and GJ creation.
Over the following year, he had multiple hospitalizations related to complications from his prior abdominal surgeries. Several EGDs throughout this time revealed severe erosive esophagitis and esophageal stenosis requiring serial dilations. He was treated with twice daily PPI therapy, although his symptoms persisted. Placement of an esophageal stent was attempted five months after the initial EGD diagnostic for esophagitis, but a subsequent rehospitalization for contained bowel perforation required this stent to be removed.
During his most recent admission, a small bowel follow-through showed marked narrowing at the GJ anastomosis site concerning for anastomotic ulcer with stricture. This area could not be traversed via EGD. A four week course of vonaprazan was prescribed upon discharge. He later underwent outpatient EGD notable for eradication of ulcer, esophageal patency, as well as complete resolution of GJ anastomotic stricturing disease. In addition, he demonstrated symptomatic improvement. Discussion: Vonoprazan has been extensively studied in progressive or untreated GERD. Marginal ulcers and gastrojejunal anastomotic strictures are common complications after gastric bypass surgery, however, the mainstay of pharamlogical therapy includes PPIs, H2 blockers, and sucralfate. When strictures occur, endoscopic dilation and surgical revision are discussed. When our surgical patient developed a refractory anastomotic ulcer with stricture and failed multiple prior PPIs, a PCAB was offered, and after only a four week treatment period, EGD revealed improvement in his symptoms as well as near-eradication of his stricturing disease.
Figure: Small bowel follow-through showing narrowing at the site of the GJ anastomosis concerning for stricture
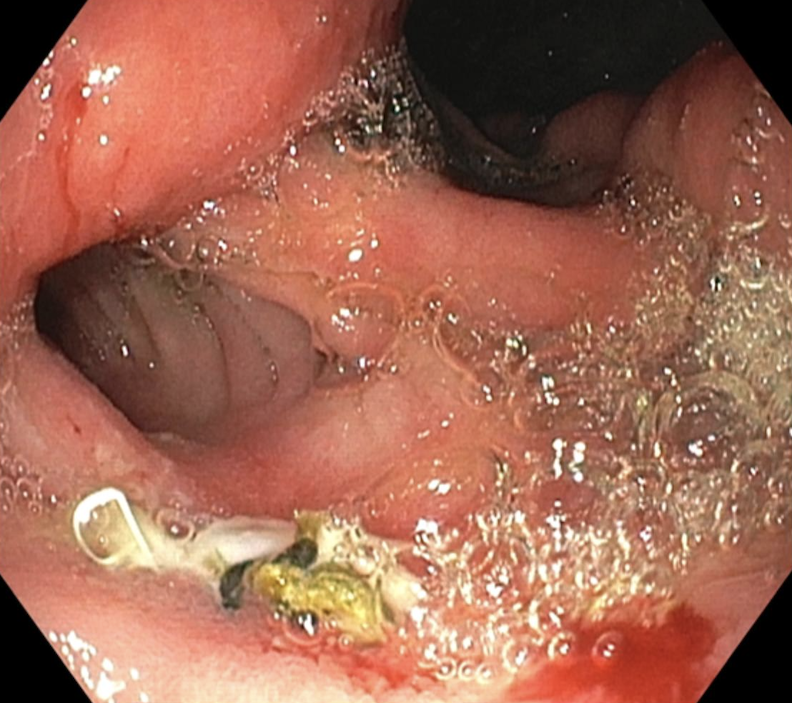
Figure: Follow-up EGD showing widely patent GJ anastomosis with intact staple line that was easily traversed compared to prior scopes
Disclosures: Casey DeBeltz indicated no relevant financial relationships. Clive Miranda indicated no relevant financial relationships. Aditya Avula indicated no relevant financial relationships. Shane Manatsathit indicated no relevant financial relationships.
Casey M. DeBeltz, DO, Clive J. Miranda, DO, MSc, Aditya Avula, DO, Shane Manatsathit, MD. P0879 - Vonaprazan Therapy Associated With Eradication of a Refractory Anastomotic Ulcer With Stricture After Gastric Bypass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.