Benjamin W. Dreskin, MD, Zachary Jurkowski, MD, MBA, Patrick J. Carey, MD, Jonathan S. Moulton, MD, Loren P. Brook, MD, MS University of Cincinnati, Cincinnati, OH Introduction: Rectal perforation is a rare but serious complication of enema insertion. Untreated, it has high morbidity and mortality. This case report describes the successful endoscopic closing of an enema-induced delayed rectal perforation using an over-the-scope clip (OTSC).
Case Description/
Methods: A 72-year-old male was admitted for observation after spinal surgery. On post-operative day 2, immediately after receiving an enema for constipation, he experienced significant rectal discomfort and abdominal pain. A CT scan of the abdomen and pelvis showed contrast extravasation concerning for anterior rectal perforation. He was afebrile and normotensive. Physical exam demonstrated mild abdominal tenderness but no signs of peritonitis. After evaluation by both gastroenterology and surgery, the decision was made to attempt endoscopic closure prior to committing the patient to surgery.
A non-bleeding perforation, approximately 7mm in diameter with surrounding mucosal congestion and edema, was identified in the rectum. Tissue edges were approximated, and an OTSC was successfully placed. This effectively closed the defect. A follow-up CT 24 hours later demonstrated improvement in pneumoperitoneum, without adjacent fluid collections or perforation. His abdominal pain improved, and he was discharged with antibiotics 4 days later without post-procedure complications. Discussion: While enemas are commonly used in the treatment of constipation, they are not without risk. A 2013 retrospective study of 269 patients given fleet enemas for acute constipation found a 1.1% incidence of rectal perforation. In a 2020 systematic review, there was a pooled mortality estimate of 38.5% among 49 patients with enema-induced rectal perforation that approached 60% for patients that were managed conservatively.
Historically, such perforations often required invasive surgical repair, including diverting colostomy, to treat relatively small defects. This patient, who was stable and without signs of peritonitis, had a subcentimeter delayed perforation that was effectively managed endoscopically. This less invasive approach likely reduced his hospital stay and had less impact on his quality of life. OTSCs are recommended for immediate management of intraprocedural colonic perforations without spillage of colonic contents into the peritoneum. This case suggests endoscopic closure with an OTSC is also a reasonable option for patients without peritonitis who experience delayed enema-induced rectal perforations.
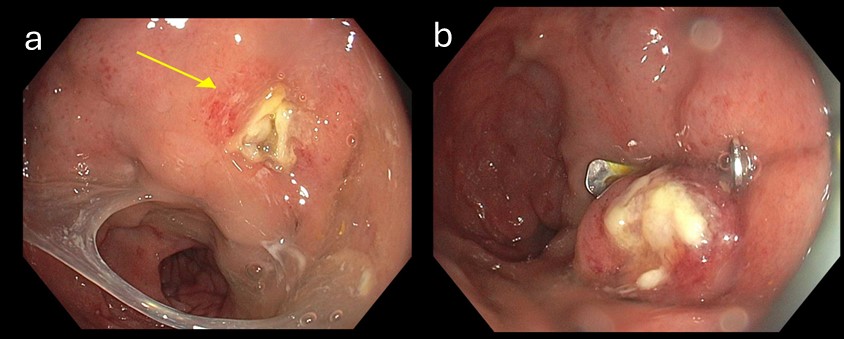
Figure: Endoscopic images of anterior rectal wall defect. (A) Rectal perforation with surrounding granulation, edema and vascular congestion. (B) Post-clipping image demonstrating closure of the defect.
Disclosures: Benjamin Dreskin indicated no relevant financial relationships. Zachary Jurkowski indicated no relevant financial relationships. Patrick Carey indicated no relevant financial relationships. Jonathan Moulton indicated no relevant financial relationships. Loren Brook indicated no relevant financial relationships.
Benjamin W. Dreskin, MD, Zachary Jurkowski, MD, MBA, Patrick J. Carey, MD, Jonathan S. Moulton, MD, Loren P. Brook, MD, MS. P0878 - When the Enema Strikes Back: Over-the-Scope Clip Closure of an Enema-Induced Rectal Perforation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Benjamin W. Dreskin, MD photo")