Washington Township Medical Group Mountain View, CA
Hiba Ghannam, MD1, Keenan Kassar, MBA2, Abdulhadi Abo Nofal, 3, Zaid Imam, MD4 1Health Point Abudhabi, Abudhabi, Abu Dhabi, United Arab Emirates; 2Loyola University, Lemont, IL; 3Alfaisal University, Riyadh, Ar Riyad, Saudi Arabia; 4Washington Hospital Healthcare System, Mountain View, CA Introduction: Acute hemorrhagic rectal ulcer syndrome (AHRU) is an emerging clinical entity first reported in Asia. AHRU can be a cause of massive painless lower gastrointestinal bleeding and is seen in critically ill patients. We hereby present a case of AHRU treated with angiography and embolization, presenting 2 years later with recurrent hemorrhage treated successfully with a combination of endoscopic and angiographic intervention. This highlights long term sequelae in a patient with AHRU and the importance of multidisciplinary care in managing the patient.
Case Description/
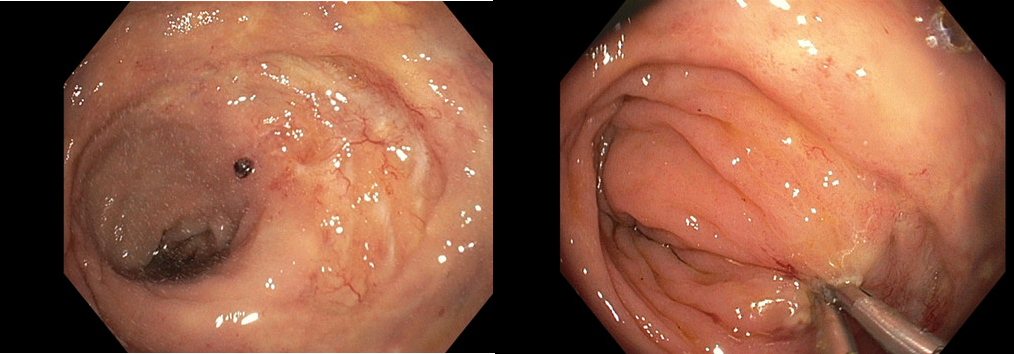
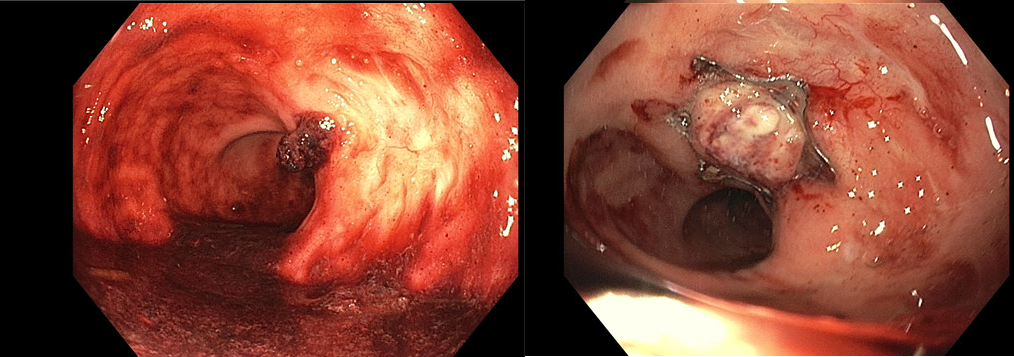
Methods: A 74-year-old-Filipino Male with medical history significant for end stage renal disease (ESRD) on hemodialysis, serous cystadenoma of the pancreas, and atrial fibrillation on anticoagulation with Apixaban was admitted with hematochezia for 2 days. He was admitted 2 years ago with similar symptoms and colonoscopy at that time showed a 32 mm hemorrhagic rectal ulcer, for which he underwent embolization of inferior mesenteric artery branches to control bleeding. Hemoglobin on his current presentation was 7.9 g/dl. The platelet count was normal. A colonoscopy was performed the following day demonstrating a healed scar in the rectum with an adjacent visible vessel and was otherwise normal. The ulcer was treated with bipolar cautery and two through the scope (TTS) hemoclips (Image 1). He was discharged but presented 3 days later with recurrent hematochezia. A repeat sigmoidoscopy was performed. The hemoclips had fallen off with recurrent hemorrhage from the same vessel. An over the scope clip (padlock device) was deployed to achieve hemorrhage control (Image 2). Given the need to resume anticoagulation, he underwent an angiogram the following day demonstrating a dominant mucosal vessel coursing towards the clip arising from the superior rectal artery. This was embolized with a series of 2 mm coils. On 2-month follow-up the patient had no recurrent bleeding or other symptoms. Discussion: We hereby present a case of AHRU presenting 2 years after the initial presentation with recurrent hemorrhage. Increased collateralization following prior embolization can be a risk factor for aberrant vessel formation. Endoscopic management with TTS clip placement was unsuccessful given clip displacement. The case additionally highlights the role of OTSC in management of refractory hemorrhage and a multidisciplinary approach to management of complex patients with lower gastrointestinal hemorrhage.
Figure: Visible vessel on initial colonoscopy (Left panel). Endoscopic result following hemoclip placement (Right panel)
Figure: Recurrent bleeding after hemoclips displaced (Left panel), Endoscopic result following over the scope clip (OTSC) placement (Right panel)
Disclosures: Hiba Ghannam indicated no relevant financial relationships. Keenan Kassar indicated no relevant financial relationships. Abdulhadi Abo Nofal indicated no relevant financial relationships. Zaid Imam indicated no relevant financial relationships.
Hiba Ghannam, MD1, Keenan Kassar, MBA2, Abdulhadi Abo Nofal, 3, Zaid Imam, MD4. P0873 - Recurrent Bleeding From Acute Hemorrhagic Rectal Ulcer Managed With an Over-the-Scope Clip Placement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.