Akira Folk, DO1, Shradha Gupta, MD2, Navroop Nagra, MD3 1Banner - University of Arizona Tucson, Tucson, AZ; 2HonorHealth, Phoenix, AZ; 3HonorHealth, Scottsdale, AZ Introduction: Dysphagia lusoria is a rare cause of esophageal compression, most commonly due to an aberrant right subclavian artery (ARSA), a congenital vascular anomaly present in 0.5–2% of the population. While often asymptomatic, esophageal compression may present later in life due to arterial stiffening or aneurysmal dilation, often leading to misdiagnosis and extensive gastrointestinal workups.
Case Description/
Methods: A 52-year-old female with a complex medical history including supraventricular tachycardia, tobacco use, depression, anxiety, and trigeminal neuropathy presented with a year-long history of persistent globus sensation and progressive neck pain. She reported worsening dysphagia and odynophagia over two weeks prior to admission. Extensive outpatient evaluations by ENT, neurology, and multiple gastroenterologists included multiple esophagogastroduodenoscopies, esophageal manometry, pH testing, and speech evaluations. These studies revealed mild pharyngeal dysphagia and gastritis but were otherwise inconclusive. Labs were notable for mild leukopenia (WBC 3.3 × 10³/µL). Imaging with CT angiogram revealed an ARSA extrinsically compressing the esophagus. A modified barium swallow demonstrated mild esophageal indentation with contrast retention at the site of vascular impingement (Figure 1). Surgical correction was considered but ultimately deferred, and the patient was discharged with close outpatient GI follow-up. Discussion: An ARSA arises from abnormal regression of the embryonic fourth right aortic arch and persistence of the right dorsal aorta. While typically asymptomatic, ARSA can cause adult-onset dysphagia due to esophageal compression by the artery itself or an associated dilated Kommerell diverticulum. Endoscopic findings are often nonspecific, frequently prompting extensive gastrointestinal evaluations. Definitive diagnosis requires vascular imaging, with CT or MR angiography offering the most accurate anatomical detail. In patients with significant symptoms, surgical correction—typically involving revascularization of the ARSA and either transection at its origin or translocation to the ascending aorta—can be curative.
Dysphagia lusoria should be considered in the differential for unexplained solid food dysphagia and odynophagia, especially when imaging suggests extrinsic esophageal compression. Early vascular imaging and multidisciplinary management, including surgery when indicated, offer excellent outcomes.
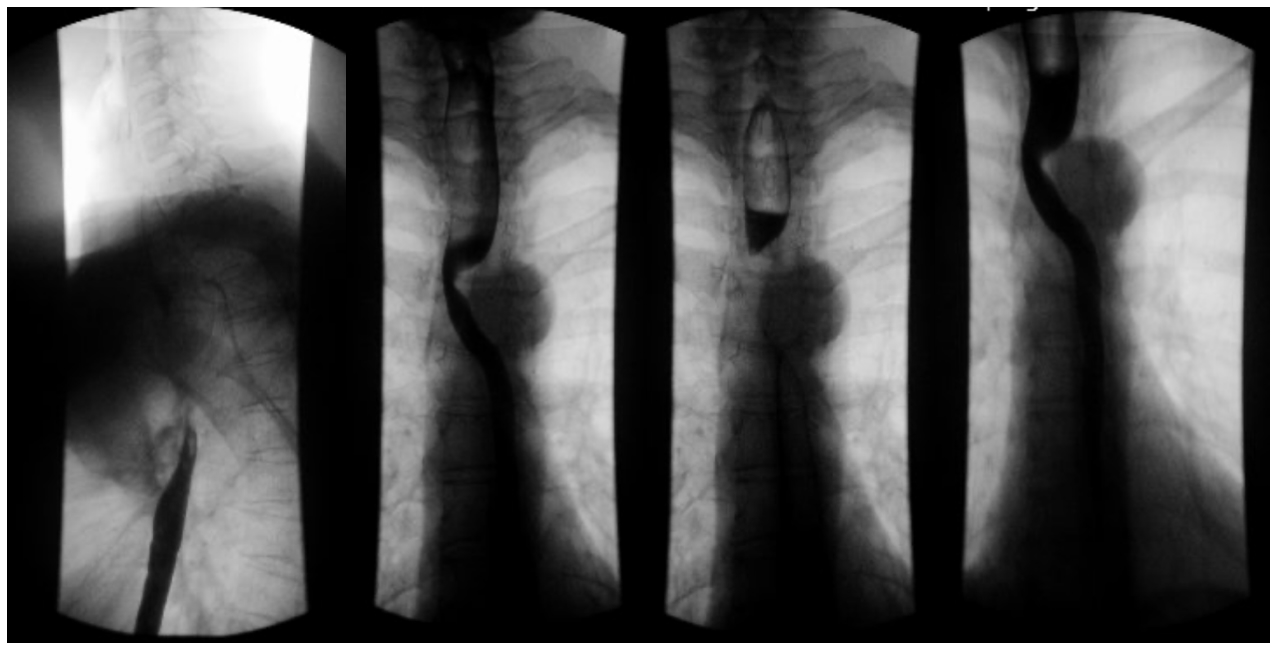
Figure: Figure 1. Esophagram showing aberrant right subclavian artery causing posterior indentation of the upper thoracic esophagus with mild contrast hold-up above the point of compression. A minimal smooth indentation is noted along the left anterolateral aspect of the distal thoracic esophagus, likely of no clinical significance. No ulceration or stricture is seen.
Disclosures: Akira Folk indicated no relevant financial relationships. Shradha Gupta indicated no relevant financial relationships. Navroop Nagra indicated no relevant financial relationships.
Akira Folk, DO1, Shradha Gupta, MD2, Navroop Nagra, MD3. P0766 - Dysphagia Lusoria in an Adult: A Rare Vascular Cause of Esophageal Dysphagia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")