Judy Alrukby, MBBS1, Yousra Eltagouri, MD2, Sofia Chaudrey, 3, Karim T.. Osman, MD2, Kristen Farwell, MD1 1Lahey Hospital and Medical Center, Burlington, MA; 2Lahey Clinic, Burlington, MA; 3Philips Exeter academy, Exeter, NH Introduction: Esophageal diverticula are rare outpouchings of the esophageal wall, often found incidentally during imaging or endoscopy. They are classified by location into Zenker’s (upper esophagus), mid-esophageal, and epiphrenic (distal esophagus) types. While most are asymptomatic or present with mild symptoms such as dysphagia or regurgitation, bleeding is an exceedingly rare complication. Proposed mechanisms including mucosal ulceration or erosion into adjacent vessels, particularly in patients on anticoagulation.
Case Description/
Methods: An 84-year-old female with paroxysmal atrial fibrillation on apixaban, heart failure with preserved ejection fraction, coronary artery disease, chronic kidney disease, and a prior left anterior resection with colostomy presented with melena noted in her colostomy bag and hemoptysis. She denied abdominal pain, nausea, or vomiting. Laboratory evaluation showed a hemoglobin of 10.1 g/dL (baseline 13.1 g/dL), hematocrit of 31.7%, and INR of 1.6. Urgent esophagogastroduodenoscopy revealed a large mid-esophageal diverticulum at 28 cm containing an adherent blood clot without active bleeding. Attempts to suction the clot were unsuccessful due to its firm adherence. Conservative management was initiated including temporary cessation of apixaban, intravenous proton pump inhibitor therapy, and serial hemoglobin monitoring. Her hemoglobin stabilized at 8.8 g/dL without transfusion, and her hemoptysis resolved spontaneously. Notably, a chest CT performed one month earlier had incidentally revealed the diverticulum. Discussion: Mid-esophageal diverticula are uncommon and rarely cause bleeding – but should be considered. A thorough review of prior imaging can provide important clues. Endoscopy remains the primary diagnostic modality. Management depends on hemodynamic status and bleeding severity. In stable patients without active bleeding, conservative management can be effective. In cases of active hemorrhage with a visible vessel, endoscopic intervention with hemostatic clips or epinephrine injection may be pursued. Thermal coagulation is another option, though its use in thin-walled esophageal diverticula is typically reserved for salvage therapy in tertiary centers with surgical backup due to the risk of perforation.
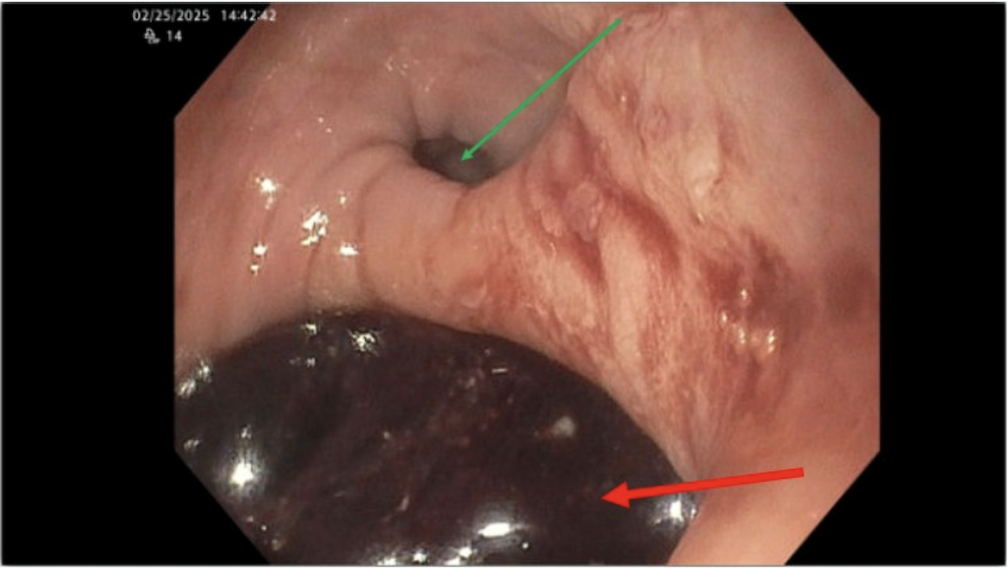
Figure: Green arrow points at esophageal lumen. Red arrow shows the large mid-esophageal diverticulum with adherent blood clot
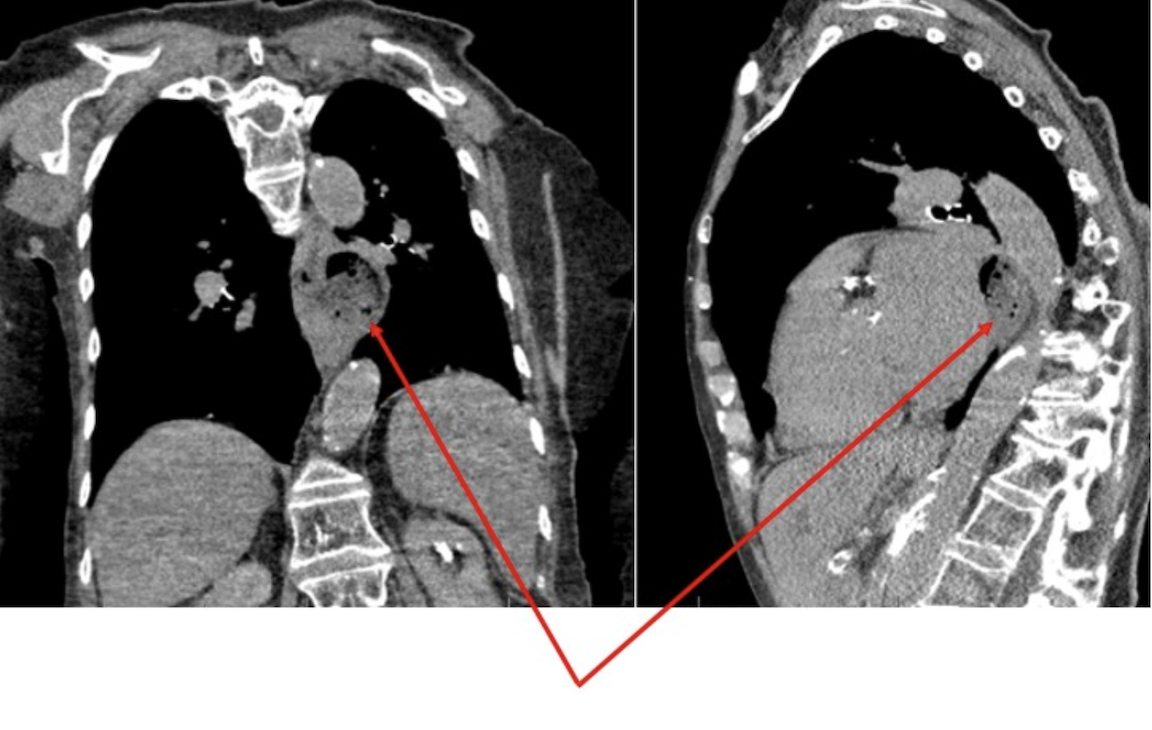
Figure: Coronal and sagittal CT images demonstrating a mid-esophageal diverticulum with associated luminal contents. The diverticulum is highlighted by red arrows.
Disclosures: Judy Alrukby indicated no relevant financial relationships. Yousra Eltagouri indicated no relevant financial relationships. Sofia Chaudrey indicated no relevant financial relationships. Karim Osman indicated no relevant financial relationships. Kristen Farwell indicated no relevant financial relationships.
Judy Alrukby, MBBS1, Yousra Eltagouri, MD2, Sofia Chaudrey, 3, Karim T.. Osman, MD2, Kristen Farwell, MD1. P0753 - Bleeding Mid-Esophageal Diverticulum: A Rare Complication Unmasked by Anticoagulation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")