Raymond Wadie, MBChB, Seth Mills, MBChB, Sohrab Zand, MBChB Cayuga Medical Center, Ithaca, NY Introduction: Acute Esophageal Necrosis (AEN) is a life-threatening condition that affects the gastroesophageal junction and is characterized by circumferential black discoloration. Risk factors for AEN include critical illness, hemodynamic instability, and underlying comorbidities that compromise perfusion or mucosal integrity. Here we describe a case of AEN caused by diabetic ketoacidosis (DKA).
Case Description/
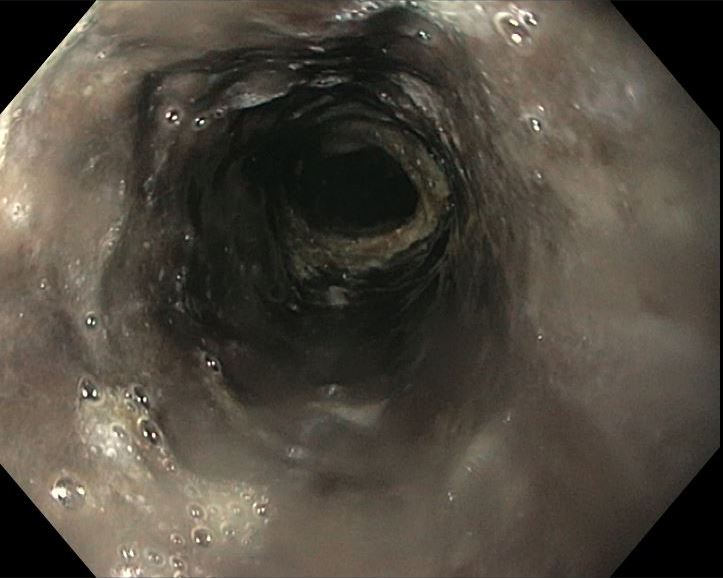
Methods: A 57-year-old male with a past medical history of diabetes mellitus presented to the emergency department with a four-day history of nausea, vomiting, malaise, and dysphagia. On arrival, he was hypotensive and tachycardic, with the initial EKG showing atrial fibrillation. Initial investigations revealed a pH of 7.16 on ABG and serum glucose of 507 mg/dl, lactate of 4.3 mmol/L, and an anion gap of 29. He was transferred to the ICU with a diagnosis of DKA and was started on continuous intravenous (IV) insulin infusion and IV fluids. Nine hours post-ICU admission, the patient had coffee-ground emesis and melena. An urgent esophagogastroduodenoscopy (EGD) revealed a circumferential black mucosa of the esophagus extending to the GE junction (Figures 1 and 2). Biopsy showed ulcerated necrotic exudate and superimposed Candida infection. The patient was made NPO and started on IV proton pump inhibitors (PPIs). Over the following days, his DKA resolved and enteral feeding was resumed. A repeat EGD four weeks after discharge revealed advanced esophageal stricture with a pinhole opening in the mid-to-distal esophagus Discussion: The etiology of AEN is multifactorial and thought to be due to tissue hypoperfusion, chemical injury, and impaired mucosal defense. To our knowledge, there has only been one other case of AEN with superimposed candida infection. This case is unique given that the underlying Candida was not treated, and management focused on treating the underlying DKA, maintaining hemodynamic stability, suppressing acid through PPI, and early enteral feeding. Although esophageal strictures may arise as a complication of AEN, the degree and severity of the stricture formation in our patient is considerable, and it is uncertain to what extent this was attributable to inadequate treatment of the underlying Candida infection. This case underlines the need for prompt recognition and aggressive management of AEN.
Figure: Distal portion of the esophagus showing a sharp demarcation at gastroesophageal junction.
Disclosures: Raymond Wadie indicated no relevant financial relationships. Seth Mills indicated no relevant financial relationships. Sohrab Zand indicated no relevant financial relationships.
Raymond Wadie, MBChB, Seth Mills, MBChB, Sohrab Zand, MBChB. P0744 - A Striking Case of Acute Esophageal Necrosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.