MedStar Georgetown University Hospital Washington, DC
Adam Khalaf, MD, Alessandro El-Khoury, MD, Ade Waterman, MBChB, Alessandra Martorella, DO, Shervin Shafa, MD MedStar Georgetown University Hospital, Washington, DC Introduction: Dysphagia lusoria is difficulty swallowing due to extrinsic esophageal compression by an aberrant subclavian artery, most commonly the aberrant right subclavian artery (ARSA). This congenital vascular anomaly, present in 0.5-2% of the population, results from abnormal development of the aortic arch. The ARSA typically courses posterior to the esophagus, leading to mechanical compression. While most individuals remain asymptomatic, 20-40% may develop symptoms. Dysphagia lusoria most commonly presents as clinical dysphagia, typically to solids and less frequently mimics gastroesophageal reflux disease (GERD), such as heartburn or regurgitation. Among those who are symptomatic, dysphagia is the predominant complaint, while GERD-like symptoms are less common. We present a case of a 21-year-old male with severe, refractory GERD and progressive dysphagia, ultimately diagnosed with ARSA-associated dysphagia lusoria.
Case Description/
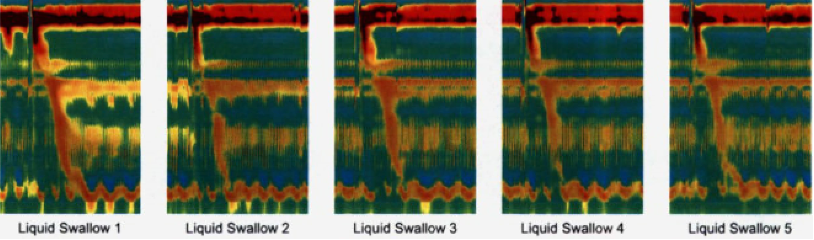
Methods: A 21-year-old male presented with six months of progressive dysphagia to solids and liquids, postprandial chest discomfort, and persistent GERD-like symptoms unresponsive to proton pump inhibitors. He also reported early satiety and exercise-induced symptom exacerbation. Endoscopic evaluation revealed a 2.5 cm hiatal hernia and inlet patches; biopsies were unremarkable. A barium esophagram demonstrated posterior indentation of the upper esophagus, concerning for extrinsic compression. Subsequent chest computed tomography angiography confirmed ARSA coursing posterior to the esophagus. Despite lifestyle and medical therapy, symptoms persisted. One year later, high-resolution manometry (Figure 1) demonstrated localized intrabolus pressurization and a pulsatile vascular band consistent with functional esophageal obstruction from ARSA, confirming dysphagia lusoria. He was subsequently referred to vascular surgery. Discussion: This case highlights a rare vascular cause of dysphagia that initially mimicked GERD. Standard diagnostic tools such as endoscopy failed to identify the etiology, with the diagnosis ultimately made through imaging and confirmed by high-resolution manometry. Notably, symptoms worsened with exercise, an uncommonly reported feature in dysphagia lusoria, possibly due to increased intrathoracic or abdominal pressure augmenting vascular compression of the esophagus. This case underscores the need to consider vascular anomalies in refractory esophageal symptoms and to maintain a broad differential when evaluating atypical GERD presentations.
Figure: Figure 1: High-resolution esophageal manometry with impedance during upright liquid swallows demonstrating focal intrabolus pressurization in the proximal esophagus, with preserved peristalsis and normal LES relaxation. The area of elevated pressure corresponds to extrinsic compression from an aberrant right subclavian artery (dysphagia lusoria), consistent with functional esophageal obstruction.
Disclosures: Adam Khalaf indicated no relevant financial relationships. Alessandro El-Khoury indicated no relevant financial relationships. Ade Waterman indicated no relevant financial relationships. Alessandra Martorella indicated no relevant financial relationships. Shervin Shafa indicated no relevant financial relationships.
Adam Khalaf, MD, Alessandro El-Khoury, MD, Ade Waterman, MBChB, Alessandra Martorella, DO, Shervin Shafa, MD. P0734 - Dysphagia Lusoria in a Young Adult: A Rare Vascular Mimic of Refractory GERD, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")