University of Texas Health, McGovern Medical School Houston, TX
Faraz Jafri, MD, MBA1, Tanvi Gupta, MD1, Eric D. Yoon, MD2, Elizabeth G. Holt, MD1 1University of Texas Health, McGovern Medical School, Houston, TX; 2McGovern Medical School at UTHealth Houston, Houston, TX Introduction: Transesophageal echocardiography (TEE) is a minimally invasive cardiac imaging technique with a low but known risk of injury to the oropharynx, esophagus, or stomach.Large case series show that the incidence of esophageal perforation after TEE is approximately 0.01-0.03%. The risk of esophageal damage may be higher during prolonged probe insertion and in structural interventions such as the placement of a Watchman device. While case reports have documented esophageal perforations and hematomas, data on esophageal tears is limited. We present a rare case of a delayed partial-thickness esophageal tear following Watchman device placement, managed successfully through endoscopy.
Case Description/
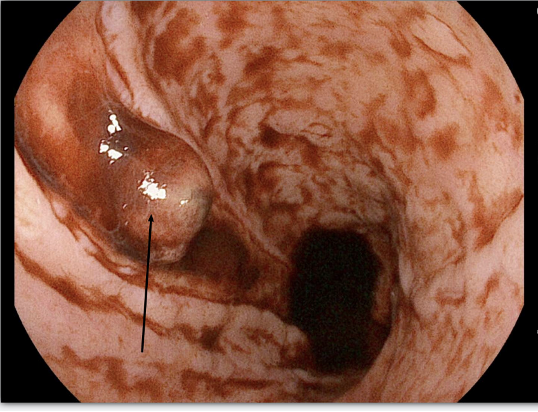
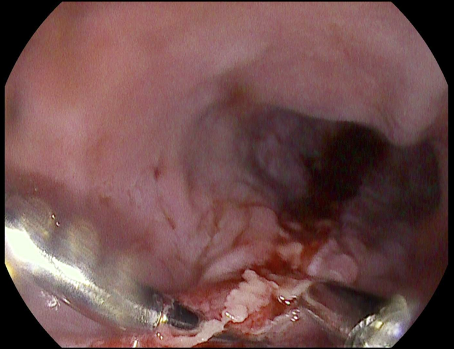
Methods: An 82-year-old female with atrial fibrillation underwent TEE-guided Watchman placement and developed hematemesis one week later. She presented after 4 episodes of large-volume hematemesis, found to be in hemorrhagic shock with a hemoglobin (Hgb) of 5.8 g/dL. Physical exam findings included pale skin, lethargic appearance, and abdominal tenderness to palpation. Massive transfusion protocol was initiated, and she was subsequently intubated for airway protection due to persistent hematemesis. Emergent esophagogastroduodenoscopy (EGD) revealed a mid-esophageal lesion, approximately 30cm from the incisor, with stigmata of recent bleeding, though visualization was limited by extensive blood and blood clots in the lower esophagus and fundus that were unable to be fully cleared (Figure 1). CTA chest showed no evidence of an aortoenteric fistula. Repeat EGD several hours later identified a partial-thickness esophageal tear, extending from the mid to distal esophagus, with a visible vessel protruding through the abnormal mucosa (Figure 2). Hemostasis was achieved after placement of 2 clips and injection of 8mL of epinephrine. The patient remained stable with a Hgb of 12.2 g/dL and no further evidence of bleeding. Discussion: This case highlights a rare but clinically significant complication of TEE. Risk factors for esophageal injury include advanced age, frailty, and prolonged probe manipulation. While most esophageal perforations occur intraoperatively, delayed presentations are possible, such as with a delayed esophageal tear. Prompt recognition and multidisciplinary care are crucial for optimal patient outcomes. Endoscopic management is preferred to stabilize bleeding and close the defects.
Figure: Figure 1: Initial EGD demonstrating a protruding blood vessel in the middle third of the esophagus.
Figure: Figure 2: Repeat EGD demonstrating successful hemostasis after placement of two clips and injection of epinephrine, closing the esophageal defect.
Disclosures: Faraz Jafri indicated no relevant financial relationships. Tanvi Gupta indicated no relevant financial relationships. Eric Yoon indicated no relevant financial relationships. Elizabeth Holt indicated no relevant financial relationships.
Faraz Jafri, MD, MBA1, Tanvi Gupta, MD1, Eric D. Yoon, MD2, Elizabeth G. Holt, MD1. P0684 - When TEE Turns Traumatic: Delayed Esophageal Tear Following Watchman Placement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.