Hospital Roosevelt / Gastri-k Guatemala City, San Marcos, Guatemala
Jorge Obando, 1, Victoria Morales, 2, Rafael Orellana, 1, Abel Sanchez, MD, MSc3 1Gastroenterology & Digestive Endoscopy Unit, Roosevelt Hospital, University of San Carlos of Guatemala, Guatemala City, Chimaltenango, Guatemala; 2Gastroenterology and Digestive Endoscopy, Roosevelt Hospital, Guatemala., Guatemala City, Chimaltenango, Guatemala; 3Hospital Roosevelt / Gastri-k, Guatemala City, San Marcos, Guatemala Introduction: Mid-esophageal diverticulum is the rarest of all known esophageal diverticula. This case report describes its clinical presentation in a resource-limited setting in Guatemala, Central America, highlighting the challenges faced and strategies employed
Case Description/
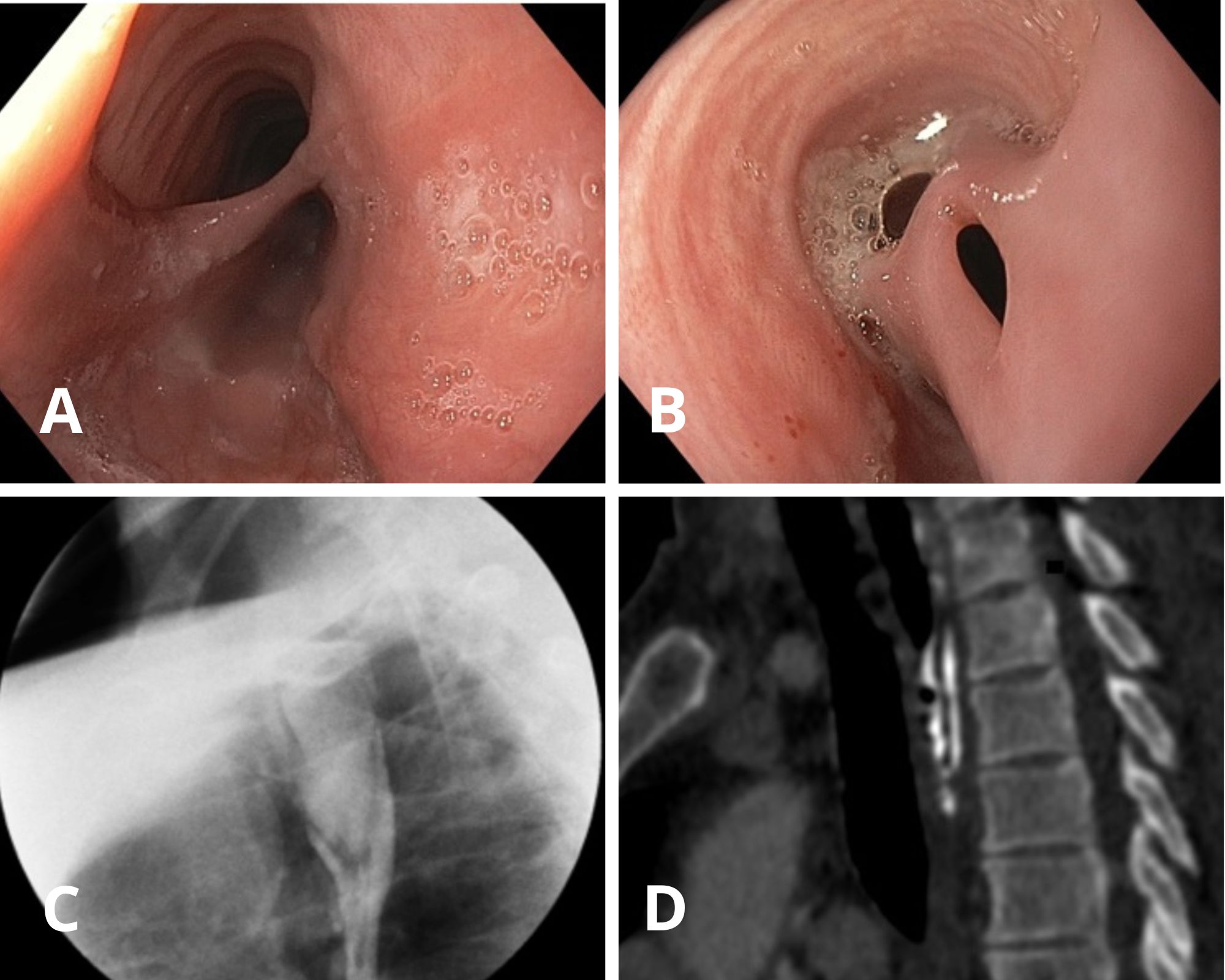
Methods: A 47-year-old male with no reported medical history presented to our public hospital with a three-month history of dysphagia, weight loss, and regurgitation. Upon admission, the patient was stable with unremarkable physical examination. Laboratory tests ruled out pulmonary tuberculosis and HIV infection. An upper endoscopy showed, at 24 cm from the dental arch, the diverticular septum, the ostium of the diverticular sac, and the esophageal lumen, along with a distal fistulous opening from the sac into the esophagus. A barium esophagram revealed a posterior saccular image in the proximal third of the esophagus, filling with contrast, measuring 18 mm in length and 34 mm in diameter, with delayed passage of contrast from the sac to the distal esophagus. A thoracic CT scan showed a filiform saccular image at the T1 level, posterior to the esophagus, extending posterolaterally to the T4 projection, with a transverse diameter of 8.1 mm, and recommunication with the main esophageal lumen. Due to limited resources, endoscopic treatment was not available. The patient was referred to thoracic surgery for esophagectomy Discussion: Mid-esophageal diverticulum is a rare condition. Risk factors such as esophageal motility disorders, mediastinal inflammatory processes, and chronic inflammation should be ruled out. Treatment depends on the diverticulum’s size and the patient's symptoms and may include surgical resection or diverticular peroral endoscopic myotomy (D-POEM), the latter associated with fewer risks and complications. In resource-limited settings, the management of mid-esophageal diverticulum relies heavily on the availability of diagnostic and therapeutic tools, as illustrated in our case, which ultimately impacts patient outcomes
Figure: Figure A. Endoscopy shows diverticular septum at 24 cm from dental arch. Figure B. Fistulous tract observed at the distal end of the diverticular sac. Figure C. Barium study shows posterior sac (18×34 mm) with delayed contrast flow. Figure D. CT scan reveals filiform diverticulum from T1 to T4 with esophageal link.
Disclosures: Jorge Obando indicated no relevant financial relationships. Victoria Morales indicated no relevant financial relationships. Rafael Orellana indicated no relevant financial relationships. Abel Sanchez indicated no relevant financial relationships.
Jorge Obando, 1, Victoria Morales, 2, Rafael Orellana, 1, Abel Sanchez, MD, MSc3. P0682 - Atypical Presentation of Mid-Esophageal Diverticulum With Esophageal Fistula: Experience From a Public Hospital in Central America, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")