Washington University School of Medicine in St. Louis / Barnes-Jewish Hospital St. Louis, MO
Allen Liu, MD Washington University School of Medicine in St. Louis / Barnes-Jewish Hospital, St. Louis, MO Introduction: Amyloidosis is a systemic illness from misfolded protein deposits commonly affecting the kidneys, heart, liver, and gastrointestinal (GI) tract. GI symptoms are often non-specific and do not trigger amyloidosis work-up. We describe a patient whose GI symptoms prompted work-up that made the diagnosis.
Case Description/
Methods: A 67-year-old man with recent Bell's Palsy and CKD presented to the hospital for syncope. Over the last 3 months, he experienced unintentional weight loss of 30 lbs (60 lbs in last 2 years), anorexia limited by dysgeusia and post-prandial nausea, and thrice daily loose stools. Stool was negative for parasites and C. difficile. Kappa and lambda free light chains were elevated with kappa/lambda (K/L) ratio 0.27. Upper endoscopy (EGD) showed intestinal metaplasia in the gastric antrum. Colonoscopy showed recto-sigmoid junction erosions. Biopsies revealed lymphoplasmacytic infiltrate in gastric body and Congo Red positive amyloid deposits in the gastric antrum, duodenum, and recto-sigmoid junction. Bone marrow biopsy revealed vascular amyloid deposits and plasmacytosis, confirmed as AL amyloid by mass spectrometry. PET-CT showed mild gastric antrum uptake. Echocardiogram did not reveal cardiac involvement. Other organs involved included kidney (albuminuria), liver (elevated INR and non-cirrhotic ascites), and nerves (Bell’s Palsy, orthostasis, dysgeusia). He developed positive C. difficle requiring extended course fidaxomicin. He started Dara-CyBorD (daratumumab, cyclophosphomide, bortezomib, dexamethasone), and K/L ratio normalized in 2 weeks. He was deficient in zinc and vitamins A, D, B1, and B6. Despite initial response, continued Data-CyBorD, tube feeds, and parenteral nutrition did not stave off worsening symptoms and renal and liver failure. Repeat EGD showed friable gastric mucosa with gastric ulcer positive for H. pylori but negative for lymphocytic cells. He ultimately transitioned to comfort care after 2.5 cycles of Dara-CyBorD. Discussion: This patient’s presentation of weight loss, nausea, and diarrhea prompted an EGD leading to a diagnosis of amyloidosis. Unfortunately, his disease was recalcitrant to Dara-CyBorD and advanced nutritional support. His quality of life was severely affected by digestive symptoms. This case highlights the need for earlier awareness of symptoms to make an earlier diagnosis. In addition to progressive organ failure, nutritional support remains a challenge of GI amyloidosis.
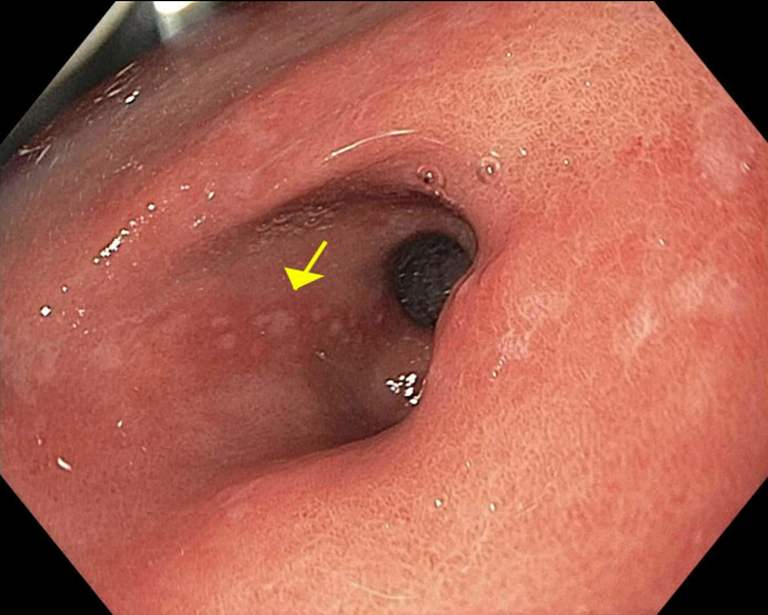
Figure: Intestinal metaplasia in the gastric antrum
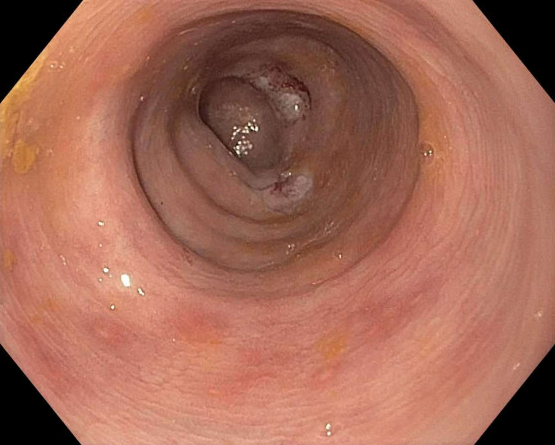
Figure: Erosions in the recto-sigmoid junction
Disclosures: Allen Liu indicated no relevant financial relationships.
Allen Liu, MD. P0575 - Gastrointestinal Symptoms Leading to Initial Recognition of Amyloidosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")