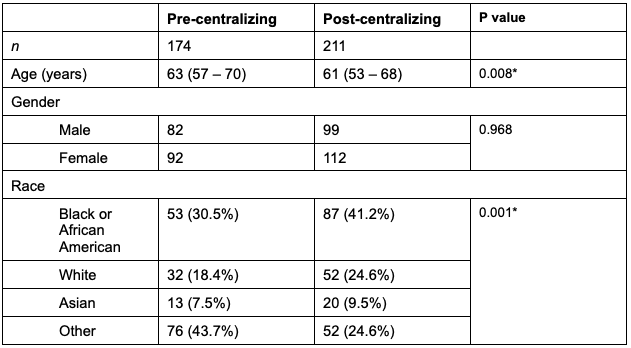
Changlin Gong, MD1, Joo Hee Park, MD2, Rahul Kumar, MD2, Kaedi Burke, MD2, Martin McIntosh, MD2, Adejoke Johnson, MD2, Donald P. Kotler, MD1 1NYC Health + Hospitals/Jacobi, Bronx, NY; 2North Central Bronx Hospital, Bronx, NY Introduction: Despite major advances in colorectal cancer prevention using colonoscopy, many people remain unscreened. Starting in 2019, a program of FIT testing was initiated in the primary care medical clinic at our hospital, which serves a disadvantaged, inner-city population. Our initial experience demonstrated a high yield of adenomas, advanced adenomas, and cancers in FIT positive (FIT+) patients studied between 2019-2021. However, a minority of the FIT+ patients underwent colonoscopy. In this follow up study, we examined the effect of centralizing the follow up management and navigation of FIT+ patients, as compared to our historical control group. Methods: In 2022, the GI patient navigators were given the responsibility for following up FIT+ results, instead of primary care providers. We retrospectively compared patients with FIT+ results from January 2022 to February 2025 (post-centralizing group) to patients who tested FIT+ from July 2019 to December 2021 (pre-centralizing group). We analyzed completion of follow-up colonoscopy, reasons for nonadherence, and colonoscopy yield. Results: Three hundred eighty five FIT+ were identified between 2019-2025, with 174 patients in pre-centralizing group and 211 in post-centralizing group. Patients in post-centralizing group were younger (mean age, 63 vs 61 years old, P = 0.008), and more African American (30.5% vs 41.2%, P = 0.001). No significant difference was found in gender. More patients in the post-centralizing group were given a colonoscopy order (75.9% vs 84.8%, P = 0.026) and completed colonoscopy (46% vs 61.6%, P = 0.001), increasing adherence by 33.4%. The effect is more clearly observed in patients for ‘screening,’ who did not have lower GI symptoms or anemia, for whom adherence rose from 41.7% to 62.5% (P = 0.001), a 49.9% increase. Reasons for nonadherence were predominantly patient-related (61.7% vs 69.1%). No significant differences were found in the timeliness of follow-up procedure, or detection rates of advanced adenoma or cancer. Discussion: Centralizing follow up and navigation improved adherence to colonoscopy in FIT+ patients by 33.4% overall, and 49.9% in patients without GI symptoms or anemia. However, 38.4% did not undergo colonoscopy, with patient refusal being the major reason. Further efforts to improve adherence through enhanced education of the implications of FIT+ are ongoing.
Figure: Table 1. Demographic characteristics
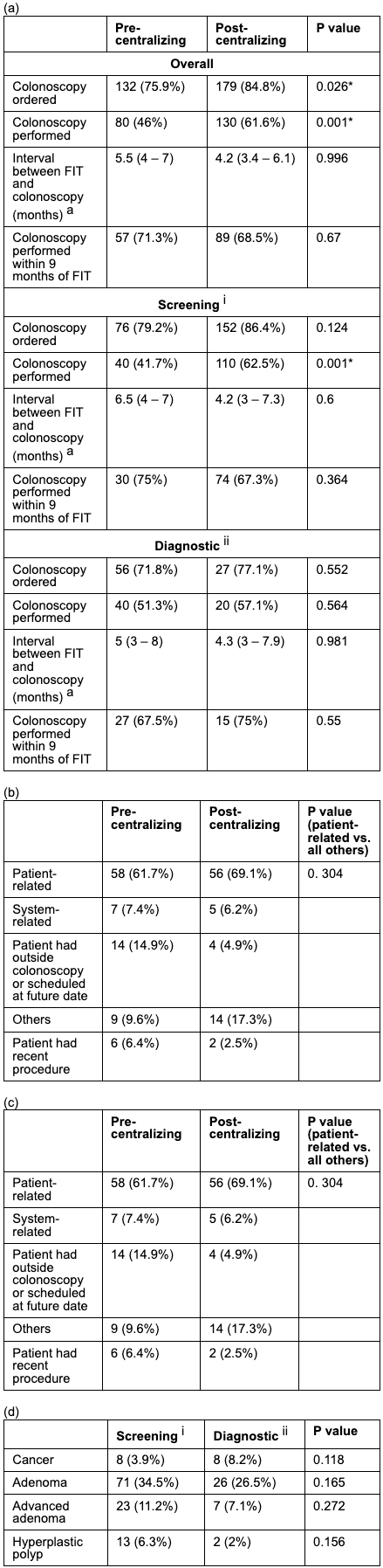
Figure: Table 2. (a) Adherence to Colonoscopy after positive FIT result, (b) Reasons for non-adherence, Yield of colonoscopy: (c) pre-centralizing vs post-centralizing (d) screening vs diagnostic; a: median value with 95% confidence interval, i: patients with no signs (such as anemia) or GI symptoms, ii: patients with signs and/or GI symptoms
Disclosures: Changlin Gong indicated no relevant financial relationships. Joo Hee Park indicated no relevant financial relationships. Rahul Kumar indicated no relevant financial relationships. Kaedi Burke indicated no relevant financial relationships. Martin McIntosh indicated no relevant financial relationships. Adejoke Johnson indicated no relevant financial relationships. Donald Kotler indicated no relevant financial relationships.
Changlin Gong, MD1, Joo Hee Park, MD2, Rahul Kumar, MD2, Kaedi Burke, MD2, Martin McIntosh, MD2, Adejoke Johnson, MD2, Donald P. Kotler, MD1. P0496 - Effects of Centralized Management of Fecal Immunochemical Test (FIT) Results on Adherence to Follow-up Colonoscopy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")