
Sunday Poster Session
Category: Colon

Arham Siddiqui, MD
University of Texas Health San Antonio
San Antonio, TX
Endoscopic biopsy is the gold standard in diagnosis and grading of colorectal cancer. In certain cases, biopsies can be false negatives due to sampling error, interpretation error, incomplete colonoscopy, and poor bowel preparation. We present an intriguing case of a patient with metastatic sigmoid adenocarcinoma with false negative biopsies due to adjacent colonic edema causing a partially obstructive mass.
Case Description/
Methods:
A 52-year-old female with no significant past medical history presented with several weeks of lower abdominal pain, difficulty passing stool, night sweats, nausea, fatigue, and a 30-pound unintentional weight loss. CT of the abdomen and pelvis showed an irregularly shaped soft tissue mass on the course of the left ureter. Follow-up MRI of the abdomen and pelvis with contrast showed a heterogeneous enhancing nodular masslike thickening of the sigmoid colon and a large exophytic component measuring 3.1 x 3.1 x 3.0 cm. Colonoscopy revealed a malignant-appearing partially obstructive mass in the proximal sigmoid colon which was soft and friable (Figures 1 and 2). Biopsy showed colonic mucosa with lamina propria edema. Colorectal surgery was consulted and laparoscopic evaluation showed a locally advanced sigmoid lesion. Patient underwent sigmoidectomy with colorectal anastomosis, omentectomy, and oophorectomy. The biopsies revealed moderately differentiated adenocarcinoma of the sigmoid colon with invasion into the visceral peritoneum and ovary. Patient was discharged with plan to start adjuvant chemotherapy.
Discussion:
The gold standard in diagnosis and grading of colorectal cancer is histopathologic analysis by endoscopic biopsy. False negative endoscopic biopsy can be due to incomplete colonoscopy, provider misinterpretation, poor bowel preparation, and inadequate biopsy. In this case, the false negative was not due to sampling or interpretation error but was uniquely caused by edema from an adjacent malignancy. There is limited literature discussing cases with similar pathophysiology. Physicians should use their clinical judgment to determine which biopsy-negative tumors should undergo surgical evaluation. Our patient presented with red flag symptoms for malignancy including weight loss and night sweats in conjunction with lower abdominal pain. Expedited confirmation of diagnosis should be of utmost importance, as colon cancer is known to metastasize in patients with or without symptoms. 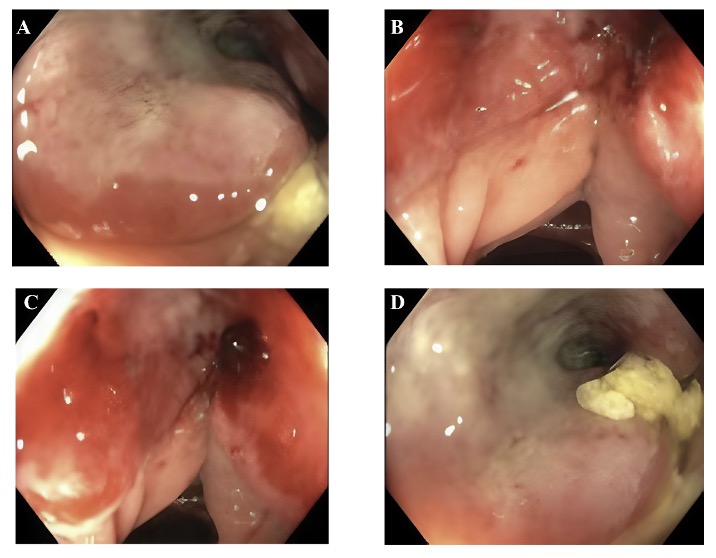
Figure: Figure 1 (A-D): Partially obstructive and friable mass in the sigmoid colon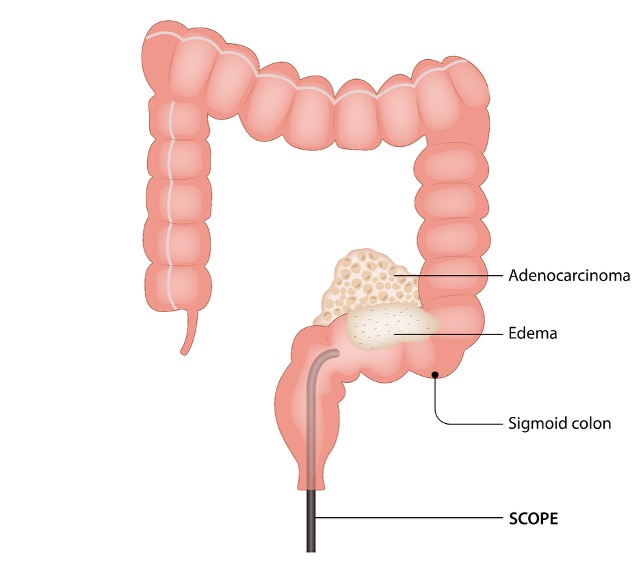
Figure: Figure 2: Partial colonic obstruction due to edema and mucus from adjacent adenocarcinoma
Disclosures:
Arham Siddiqui indicated no relevant financial relationships.
Jose De Arrigunaga indicated no relevant financial relationships.
Jason Chen indicated no relevant financial relationships.
Aaron Jabir indicated no relevant financial relationships.
Mark Shokralla indicated no relevant financial relationships.
Erin Spengler indicated no relevant financial relationships.
Arham Siddiqui, MD, Jose I.. De Arrigunaga, DO, Jason N. Chen, MD, Aaron Jabir, MD, Mark Shokralla, DO, Erin Spengler, MD. P0439 - Hidden Malignancy: A Report of False Negative Biopsy of Sigmoid Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.