Sunday Poster Session
Category: Colon

Erin Hollis, DO
Lankenau Medical Center
Wynnewood, PA
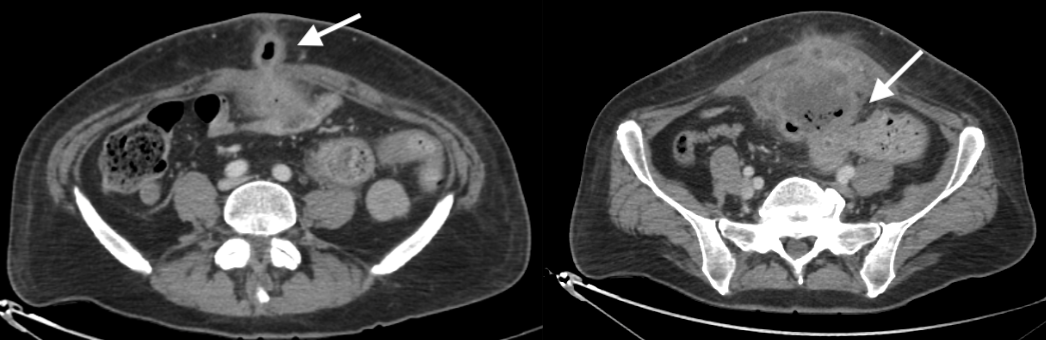
A 58-year-old male presented with a two-week history of a painless lower abdominal lump, with purulent drainage from his umbilicus. CT of the abdomen and pelvis revealed a large 14.7 x 7.5 x 10.4 cm ill-defined mass with peripheral enhancement and internal gas contiguous with the bladder dome and invading the anterior abdominal wall and umbilicus, concerning for a necrotic neoplasm (Figure). The neoplasm was suspicious for malignancy, either from a urachal remnant or a transitional cell carcinoma of the bladder. The mass was also seen to abut the anterior wall of the sigmoid colon, which could indicate either local invasion or a mass originating from the bowel wall. The patient was afebrile and labs revealed mild leukocytosis. Urine and blood cultures were obtained, as well as culture from the umbilical drainage fluid, and the patient was initiated on IV antibiotics. The patient was evaluated by general surgery, urology, and infectious disease. MRI of the abdomen & pelvis was obtained, and like his CT it was unable to differentiate between a urachal remnant malignancy or primary colon malignancy with extraluminal extension.
The patient underwent cystoscopy which revealed a large necrotic mass emanating from the bladder dome. He then underwent colonoscopy which revealed a large polypoid nearly obstructing mass in the sigmoid colon, and biopsies showed moderately differentiated urachal adenocarcinoma. Patient then underwent open urachal mass excision with partial cystectomy, sigmoidectomy, and small bowel resection with primary anastomosis. He subsequently initiated adjuvant treatment by oncology with folinic acid, fluorouracil, and oxaliplatin (FOLFOX).