McGaw Medical Center of Northwestern University Chicago, IL
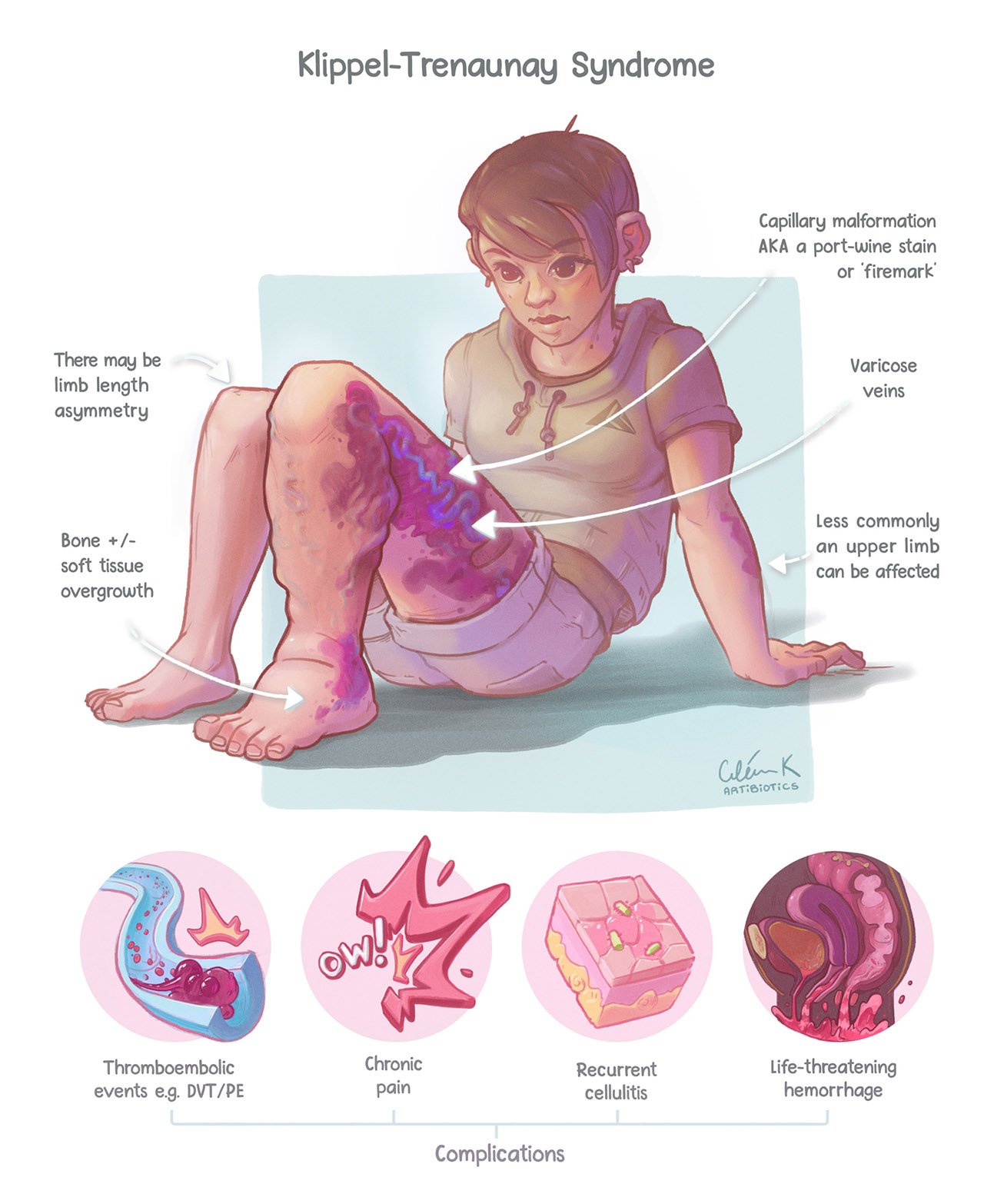
Anuragh Gudur, MD1, Krishna Kothamasu, DO2, Laurens Janssens, MD1 1McGaw Medical Center of Northwestern University, Chicago, IL; 2Jefferson Health, Philadelphia, PA Introduction: Klippel-Trenaunay Syndrome (KTS) is a rare congenital disorder involving vascular malformations driven by unchecked mTOR activation. Patients develop cutaneous capillary malformations, venous varicosities, and soft tissue hypertrophy in lower limbs. GI involvement of KTS is uncommon, but has significant morbidity and mortality.
Case Description/
Methods: A 23-year-old male with KTS presented with hematochezia for 3 weeks. Lab findings revealed microcytic anemia (Hgb 2.9 g/dL, MCV 59 fL) and iron deficiency (Ferritin 1.7 ng/mL, transferrin saturation 2%).
He had multiple manifestations of KTS since infancy, including subcutaneous varicose veins, lymphedema of the left leg, and asymmetric soft tissue overgrowth of the left foot. He was prescribed sirolimus (mTOR inhibitor) since age 6.
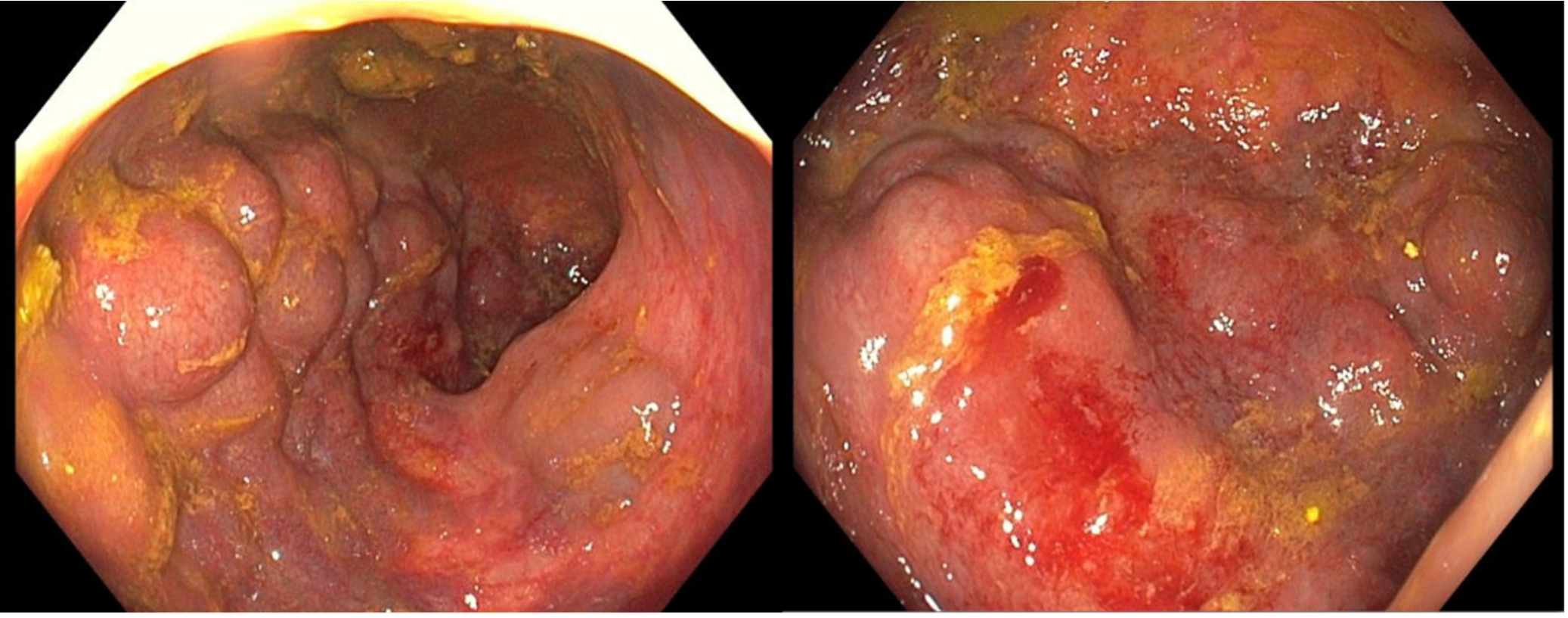
After resuscitation with blood, he underwent colonoscopy showing large dilated vascular malformations with friability in the rectum, sigmoid, and descending colon. The rectosigmoid colon had recent stigmata of bleeding.
MRI/MRV of the Abdomen/Pelvis demonstrated multifocal mass-like venous malformations in the rectum, sigmoid, and descending colon. Additional foci of venous malformations were seen in the pelvis with extension into the left thigh.
Catheter venography and angiography revealed a network of venous malformations involving sigmoid colon to the anorectal junction. There was no arterial enhancement to suggest arterial inflow or A-V shunting. IR did not identify any targets for intervention including embolization and sclerotherapy. Surgery was consulted to evaluate for sigmoidectomy. Unfortunately, the patient suffered sudden cardiac arrest (PEA) and did not achieve ROSC despite CPR. Cause of death is unknown; an autopsy is pending. Discussion: Rarely, KTS involves visceral organs, such as the colon. Patients are also at high risk of VTE and spontaneous intracerebral hemorrhage. Colonic vascular malformations carry high bleeding risk. If disease is limited to the rectum, patients receive conservative management with stool softeners, iron supplementation, and blood transfusion. Sirolimus can also slow the progression of KTS. Endovascular procedures, including sclerotherapy, or trans-anal endorectal pull-through may be performed if medical management fails. Sigmoidectomy is preferred for sigmoid disease, due to involvement of the IMV and portal vein possibly resulting in portal hypertension; sclerotherapy is avoided as this can worsen portal hypertension.
Figure: Source: Valery L. Turner, Ciléin Kearns, Kapil Wattamwar, and Anna Sophia McKenney RadioGraphics 2022 42:6, E167-E168
Figure: Left: Venous malformations in sigmoid colon Right: Venous malformations in rectum
Disclosures: Anuragh Gudur indicated no relevant financial relationships. Krishna Kothamasu indicated no relevant financial relationships. Laurens Janssens indicated no relevant financial relationships.
Anuragh Gudur, MD1, Krishna Kothamasu, DO2, Laurens Janssens, MD1. P0425 - Klippel-Trenaunay Syndrome (KTS): An Unusual Case of GI Involvement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.