
Sunday Poster Session
Category: Colon


Rishika Trivedi, MD
DHR Health
McAllen, TX
Mixed neuroendocrine-non-neuroendocrine neoplasms (MiNENs) of the colon are exceedingly rare, accounting for less than 1% of colorectal tumors. Their dual histology, often combining adenocarcinoma and neuroendocrine carcinoma, presents diagnostic and therapeutic challenges. We present a unique case of colorectal MiNEN with mucinous adenocarcinoma and large cell neuroendocrine carcinoma components.
Case Description/
Methods: A 74-year-old woman with hypertension and hyperlipidemia was referred for evaluation of iron-deficiency anemia. She denied overt gastrointestinal bleeding but reported increased fatigue. Colonoscopy revealed two adjacent lesions in the distal transverse colon: a large circumferential mass approximately 60 cm from the anal verge and a smaller polypoid lesion 5 cm proximally. Biopsy of the larger lesion showed poorly differentiated large cell neuroendocrine carcinoma with a Ki-67 index >90%, prompting urgent oncologic referral. She underwent laparoscopic extended right hemicolectomy with intraoperative tattoo localization. Gross examination revealed a 6.3 × 4.5 cm tumor infiltrating through the colonic wall (Figure 1). Final pathology demonstrated a rare mixed neuroendocrine-non-neuroendocrine neoplasm (MiNEN), composed of well-differentiated mucinous adenocarcinoma and high-grade large cell neuroendocrine carcinoma. One of twelve lymph nodes was positive for metastatic mucinous carcinoma. Margins were negative; no lymphovascular or perineural invasion was noted. The tumor was staged as pT3N1a. Immunohistochemistry showed loss of MLH1 and PMS2 with intact MSH2/MSH6, confirming Mismatch Repair Deficiency (dMMR). Focal chromogranin and synaptophysin expression supported neuroendocrine differentiation. She completed 12 cycles of adjuvant FOLFOX. Follow-up PET/CT scans at 6 and 12 months showed no recurrence.
Discussion: This case highlights the exceptional rarity of colorectal MiNEN with both mucinous adenocarcinoma and large cell neuroendocrine carcinoma components. The coexistence of dual aggressive histologies presents a unique therapeutic challenge and complicates standard management and surveillance algorithms. As long-term outcomes remain unclear, this case reinforces the importance of close multidisciplinary follow-up and contributes to the limited literature on these complex malignancies.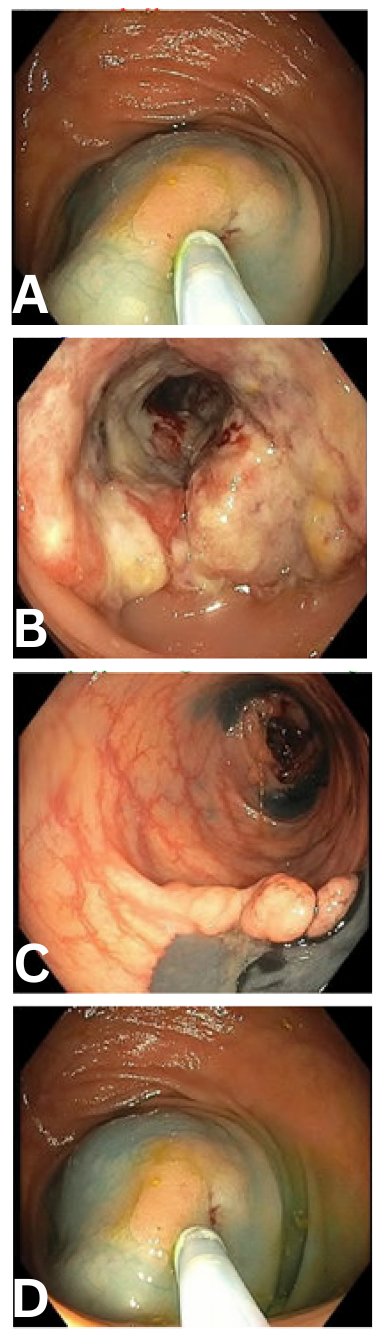
Figure: Figure 1: Representative colonoscopic images from index evaluation.
(a) A 2 cm flat polyp in the cecum, resected via hot snare polypectomy after submucosal lift.
(b) A large, circumferential, infiltrative lesion in the distal transverse colon approximately 60 cm from the anal verge; biopsy was taken, and the distal margin was tattooed with India ink.
(c) A second polypoid lesion located at 55 cm from the anal verge, adjacent to the primary mass; distal margin also tattooed.
(d) Repeat view of the cecal polyp post-lift and tattoo.
Disclosures:
Rishika Trivedi indicated no relevant financial relationships.
Mahmoud Barbarawi indicated no relevant financial relationships.
Prince Shah-Riar indicated no relevant financial relationships.
Prateek Harne indicated no relevant financial relationships.
Arturo Suplee indicated no relevant financial relationships.
Asif Zamir indicated no relevant financial relationships.
Rishika Trivedi, MD1, Mahmoud Barbarawi, MD1, Prince Shah-Riar, MD2, Prateek Harne, MD3, Arturo Suplee, MD4, Asif Zamir, MD, FACG5. P0397 - A Rare Case of Colonic MiNEN: Coexisting Large Cell Neuroendocrine Carcinoma and Mucinous Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.