SUNY Downstate Health Sciences University Brooklyn, NY
Award: ACG Presidential Poster Award
Anita H. Nguyen, MD1, Sushil K. Ahlawat, MD2 1SUNY Downstate Health Sciences University, Brooklyn, NY; 2SUNY Downstate Medical Center, Brooklyn, NY Introduction: Prostate cancer, the second most common malignancy in men, typically metastasizes to the bone, lung, or liver. Direct spread to the rectum is uncommon due to separation by a fascial plane. We present a case of prostate cancer that was diagnosed via colonoscopy.
Case Description/
Methods: A 69-year-old-man presented to primary care complaining of difficulty urinating and bothersome hemorrhoids and was referred accordingly. Cystoscopy and transrectal US showed prostatomegaly and PSA was mildly elevated at 10 ng/mL. CT urogram showed a 10 cm prostatic mass with loss of fat plane between the bladder and rectum suspicious for tumor invasion, but outside MRI suggested that the mass was external and invading the prostate. CEA was normal. The patient had missed his initial colorectal surgery and GI referrals, but eventually followed up after encouragement by urology. He had developed progressive constipation, hematochezia, and rectal pain over months which he had ascribed to hemorrhoids. Large non-bleeding external hemorrhoids were noted on exam. Colonoscopy revealed a large anterior rectal mass occupying almost the entire vault, 1-2 cm from the anal verge. It was firm on digital palpation but friable on biopsy and spontaneously oozing. Histology revealed poorly differentiated carcinoma that was positive for NKX3.1 but negative for CDX2, CK5/6, and P16 which was consistent with prostatic origin. Discussion: This case highlights the diagnostic pitfalls that can occur in this rare presentation of prostate cancer, especially from the perspective of a gastroenterologist evaluating rectal lesions. Our case had the benefit of multiple clinical elements pointing toward prostate involvement of the rectal mass including cross-sectional imaging and urinary retention. However, urinary retention and modest PSA elevation is more often due to benign prostatic hyperplasia and cross-sectional imaging is not always indicated. Furthermore, large external hemorrhoids which can present with rectal pain and hematochezia exacerbated by constipation. It is important to note that although our patient was found to have a large, distinct, partially obstructing anterior rectal mass, the endoscopic appearance can be widely variable, ranging from an ulcerated lesion to a circumferential stenotic mass. Recognition of this rare entity is essential for prompt diagnosis. Immunohistochemical staining for prostate markers may not be routinely performed for rectal specimens, so suspicions should be conveyed to the pathologist accordingly.
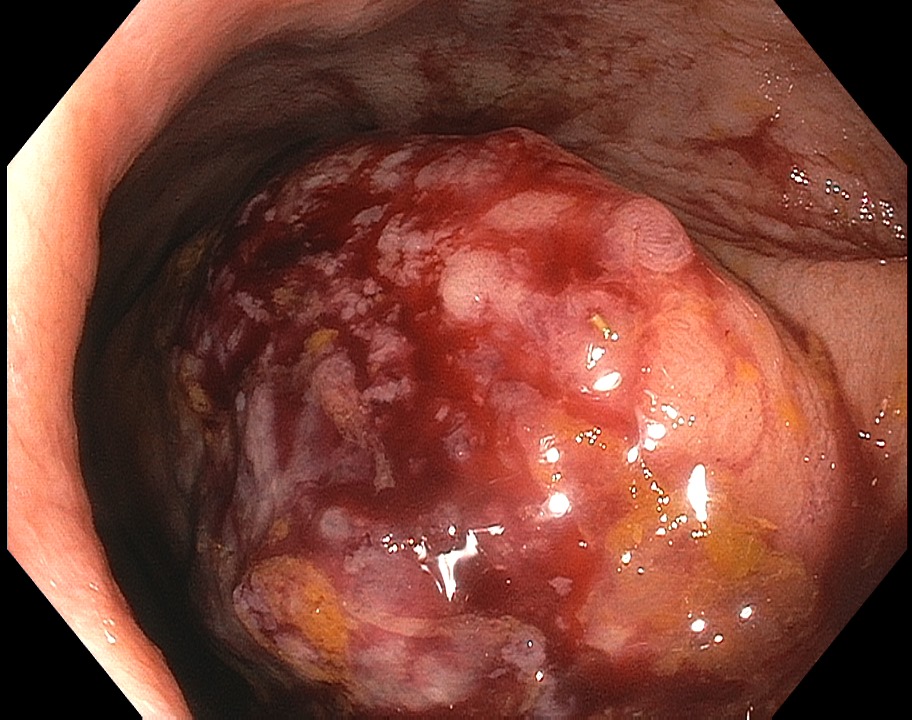
Figure: Rectal mass on initial colonoscopy view, prior to biopsy or advancement of scope.
Figure: CT urogram showing large heterogenous mass involving prostate and rectum.
Disclosures: Anita Nguyen indicated no relevant financial relationships. Sushil Ahlawat indicated no relevant financial relationships.
Anita H. Nguyen, MD1, Sushil K. Ahlawat, MD2. P0349 - Prostate Cancer Masquerading as a Rectal Tumor, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



.jpg "Anita H. Nguyen, MD (she/her/hers) photo")