Hobie L. Hughes, DO1, Lauren Healey, DO2, Nathaniel Winstead, MD, MSPH, FACG1, Jonathan Francis, MD1, Matthew Eves, MD1, Seyed Javid Taghados, MD1, Kelsey Dombrowski, DO1 1Thomas Hospital, Fairhope, AL; 2University of South Alabama, Mobile, AL Introduction: Foreign body ingestion is rare in adults compared to children and is often accidental, accounting for over 95% of cases. Accidental foreign body ingestion in adults tends to occur more often in the elderly, individuals with underlying psychiatric conditions, and during acute alcohol intoxication. The typical culprit is usually food related, such as fish or chicken bones, and most pass without the need for intervention. Endoscopic intervention is required in only about 10-20% of cases, and surgical intervention is required in less than 1% of cases. The esophagus is the most frequent site of obstruction in the gastrointestinal (GI) tract, often becoming impacted at sites of physiologic or pathologic luminal narrowing. It is rare for an orally ingested foreign body to pass through the entire GI tract and reach the colon. However, when it occurs it requires prompt evaluation and removal to avoid further complications.
Case Description/
Methods: A 56-year-old male with a history of gastroesophageal reflux disease, incision hernia repair, and colonic mass status post partial colectomy presented for evaluation of worsening abdominal pain over the past month and abnormal computed tomography (CT) imaging. CT of the abdomen and pelvis showed mild inflammatory changes along the mid transverse colon along a possible previous suture site but could not rule out a possible foreign body. Gastroenterology was consulted, and he underwent an esophagogastroduodenoscopy (EGD) and colonoscopy. The EGD was unremarkable. The colonoscopy showed evidence of a foreign body at the colonic anastomosis with successful removal of a small chicken bone. Discussion: The majority of foreign bodies ingested orally typically either pass uneventfully in most cases or cause complications in the upper GI tract prompting intervention. While it is rare for foreign body impaction or obstruction to occur in the lower GI tract from an orally ingested item, chances of this occurring increase in patients with certain risk factors. One such risk factor present in this case would be this patient’s history of a colonic mass requiring resection and creation of a colonic anastomosis which was found to be the site of impaction. A diagnosis of foreign body ingestion requires thorough history taking and a broad approach when creating a differential diagnosis. Imaging modalities are frequently used to rule out complications such as obstructions, perforations, or fistulas and can dictate whether endoscopic of surgical intervention is necessary.
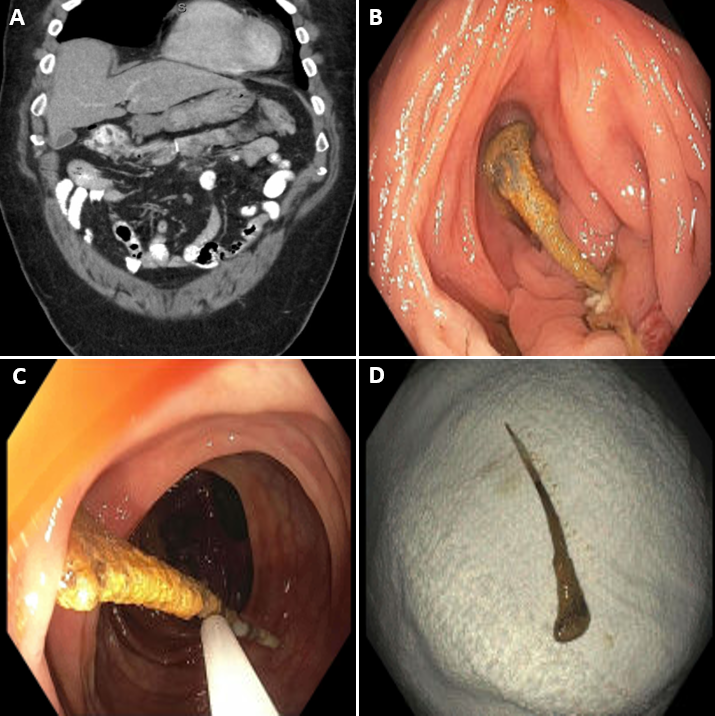
Figure: A: Coronal view of CT abd/pelvis showing mild colonic inflammation with evidence of previous anastomotic suture vs foreign body in the mid-transverse colon. B: Colonoscopic view of foreign body at previous mid-transverse colon anastomosis site. C: Process of removal of foreign body using cold snare. D: Displayed foreign body after successful removal.
Disclosures: Hobie Hughes indicated no relevant financial relationships. Lauren Healey indicated no relevant financial relationships. Nathaniel Winstead indicated no relevant financial relationships. Jonathan Francis indicated no relevant financial relationships. Matthew Eves indicated no relevant financial relationships. Seyed Javid Taghados indicated no relevant financial relationships. Kelsey Dombrowski indicated no relevant financial relationships.
Hobie L. Hughes, DO1, Lauren Healey, DO2, Nathaniel Winstead, MD, MSPH, FACG1, Jonathan Francis, MD1, Matthew Eves, MD1, Seyed Javid Taghados, MD1, Kelsey Dombrowski, DO1. P0342 - Fowl Play: Successful Colonoscopic Extraction of a Chicken Bone, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")