
Sunday Poster Session
Category: Colon


Neal K. Bhachawat, DO
Houston Methodist Hospital
Houston, TX
Septic thrombophlebitis of the portal venous system is a rare complication of intra-abdominal infections. Involvement of the inferior mesenteric vein (IMV) is even less common. We present a case of septic thrombophlebitis secondary to sigmoid diverticulitis, with early imaging revealing gas in the IMV and subsequent bacteremia.
Case Description/
Methods:
A 47-year-old man with a history of Sjögren’s syndrome, rheumatoid arthritis (on mycophenolate), and type 2 diabetes mellitus presented with several days of abdominal pain, nausea, vomiting, and diarrhea. He was hemodynamically stable but met criteria for sepsis. On exam, he had a soft, distended abdomen with diffuse tenderness. Labs showed hypokalemia (3.1 mEq/L), hyponatremia (131 mEq/L), bicarbonate of 16 mEq/L, and a normal lactate. CBC revealed neutrophilic leukocytosis (11.17 k/μL) and normocytic anemia (Hgb 11.2 g/dL). Initial blood cultures were negative. CT abdomen/pelvis with IV contrast showed sigmoid diverticulitis with localized perforation and gas in the IMV extending toward the splenomesenteric venous confluence and portal vein (image 1). He was started on IV piperacillin-tazobactam and fluconazole. Conservative treatment was pursued. On hospital day five, symptoms and sepsis persisted. Repeat CT abdomen/pelvis with IV contrast showed a diverticular abscess and IMV thrombophlebitis with extension into the splenic vein (image 2). Blood cultures were now positive for Escherichia coli with high MIC to piperacillin-tazobactam; antibiotics were changed to meropenem. Follow-up cultures 48 hours later were negative. The abscess was deemed too small for drainage. Hematology recommended therapeutic apixaban for 3–6 months, as the thrombosis was provoked. The patient improved clinically, tolerated diet, and was discharged with a PICC line for 4 weeks of ertapenem and oral fluconazole. Mycophenolate was held. Follow-up imaging was planned post therapy, but the patient was lost to follow-up.
Discussion:
Septic IMV thrombophlebitis is rare but serious. Awareness of this complication is critical for early diagnosis and management. Imaging may show gas in the venous system before thrombosis. Blood cultures can be positive and help guide management. This case highlights the importance of recognizing early radiologic signs of septic thrombophlebitis in the setting of diverticulitis. Prompt diagnosis and treatment involving antimicrobial therapy and anticoagulation can lead to favorable outcomes.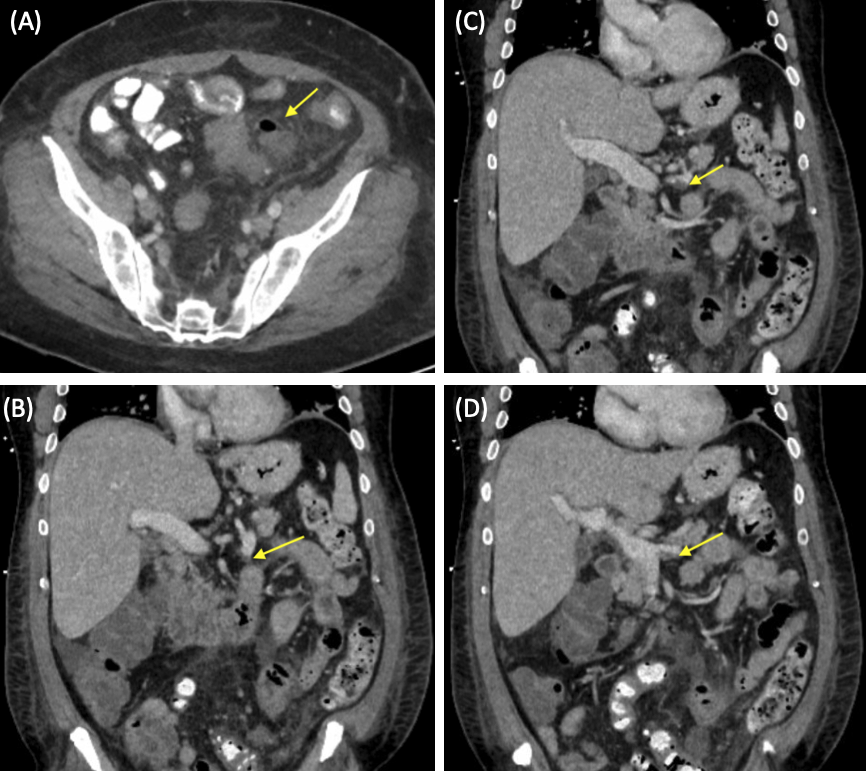
Figure: Image 1 Compute Tomography (CT) abdomen/pelvis with intravenous contrast: (A) coronal view shows sigmoid diverticulitis (yellow arrow) with localized perforation (white arrow). (B) axial view shows air in the inferior mesenteric vein (arrow). (C) coronal view shows air in the inferior mesenteric vein (arrow).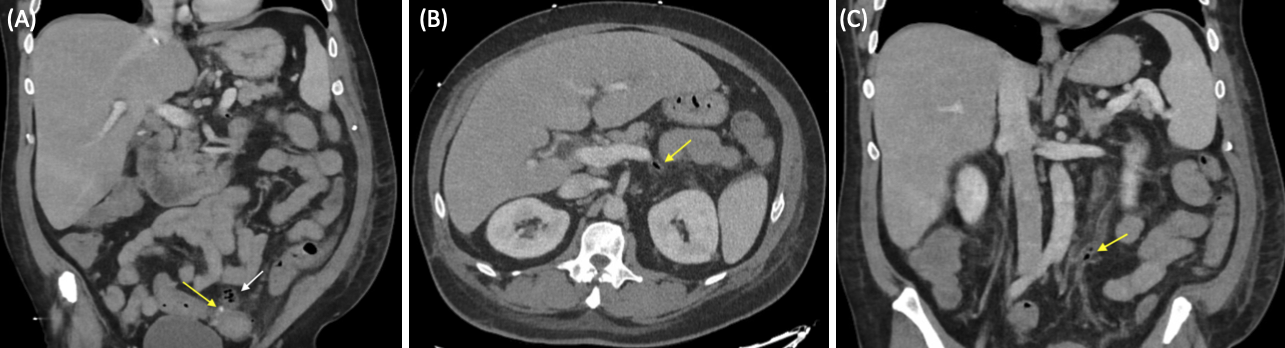
Figure: Image 2 Compute Tomography (CT) abdomen/pelvis with intravenous contrast: (A) axial view shows a diverticular abscess (arrow). (B) coronal view shows a thrombus in the inferior mesenteric vein (arrow); (C-D) coronal view shows extension of thrombus into the splenic vein (arrow).
Disclosures:
Neal Bhachawat indicated no relevant financial relationships.
Siddarth Das indicated no relevant financial relationships.
Aron Bhachawat indicated no relevant financial relationships.
Neal K. Bhachawat, DO1, Siddarth Das, DO1, Aron Bhachawat, BBA2. P0340 - Inferior Mesenteric Vein Thrombophlebitis Secondary to Diverticulitis: Early Radiologic Clues and Management, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.