Kirk Kerkorian School of Medicine at the University of Nevada Las Vegas Las Vegas, NV
Magnus Chun, MD1, Scott Diamond, DO2 1Kirk Kerkorian School of Medicine at the University of Nevada Las Vegas, Las Vegas, NV; 2Utah Gastroenterology, St. George, UT Introduction: Common sites of metastasis for advanced prostate cancer are the bone, lymph nodes, and liver parenchyma.1 It is rare for patients to develop obstructive jaundice from extra-hepatic biliary duct obstruction (3%) with non-hodgkin lymphoma (1%) and adenopathy (.6%) being the least common.2 We present a case of advanced metastatic prostate cancer to lymph nodes causing obstructive jaundice from adenopathy externally compressing the bile ducts.
Case Description/
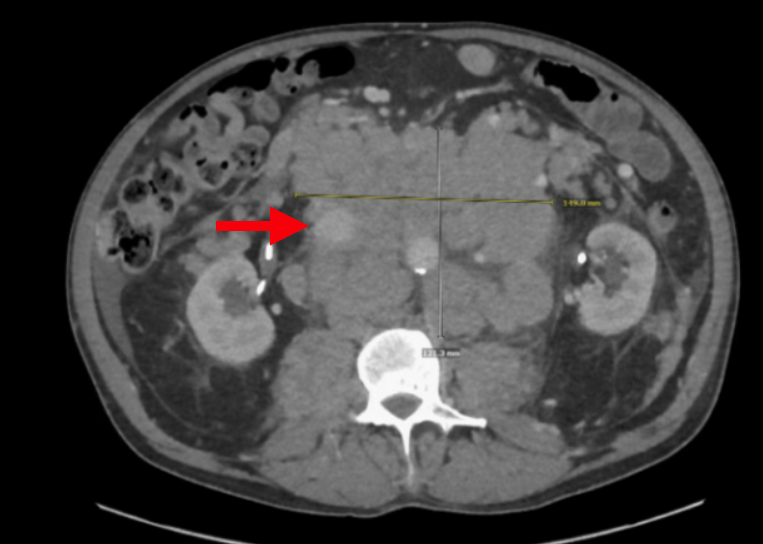
Methods: A 68-year-old male with biopsy confirmed metastatic prostate cancer to the retroperitoneal lymph nodes with secondary obstructive uropathy requiring renal replacement therapy presented with new-onset jaundice, dull abdominal pain, nausea, and constipation. He was on hormone suppressive treatment with bicalutamide and leuprolide. Examination revealed generalized jaundice, scleral icterus, and tenderness to palpation on the right upper quadrant. Pertinent labs included total bilirubin of 17.4 mg/dL, alkaline phosphatase of 1091 IU/L, ALT of 212 IU/L, and AST of 248 IU/L. His PSA was 310 ng/mL. CT abdomen and pelvis with IV contrast revealed severe intra- and extrahepatic bile duct dilation with obstruction from adenopathy. The liver had normal contour without any masses (Figure 1). It also revealed extensive bulky retroperitoneal and gastrohepatic adenopathy with bilateral pelvic adenopathy (Figure 2). The patient was offered palliative stenting of the bile duct, however, he opted for hospice care instead. Discussion: Obstructive jaundice from prostate cancer without liver parenchymal metastases is rare with three previously documented case reports.3-5 Patients with secondary biliary obstruction from metastatic adenopathy have high mortality due to a lower chance of reversible cholestasis from high tumor burden compared to primary metastatic disease of the liver.6,7 Clinicians should suspect biliary obstruction from prostate cancer metastasis if a patient's PSA is > 100 ng/mL as this is a proxy for metastatic disease, prompting further imaging evaluation.8 Treatment should be directed to relieve symptoms palliatively with biliary stent placement. For advanced disease, covered metallic stents are more effective than plastic stents.9,10 It is important to differentiate between obstructive jaundice in prostate cancer from a more common hepatic metastasis, as compared to external compression from adenopathy because of the prognostic implications. Understanding this should guide clinical decision making and patient goals of care discussions.
Figure: Figure 1. CT abdomen/pelvis with IV contrast revealed severe intra- and extrahepatic bile duct dilation with obstruction from adenopathy.
Figure: Figure 2.CT abdomen/pelvis with IV contrast revealed extensive bulky retroperitoneal and gastrohepatic adenopathy with bilateral pelvic adenopathy.
Disclosures: Magnus Chun indicated no relevant financial relationships. Scott Diamond indicated no relevant financial relationships.
Magnus Chun, MD1, Scott Diamond, DO2. P0250 - A Rare Case of Metastatic Prostate Cancer Causing Obstructive Jaundice, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.