University of Colorado Anschutz Medical Campus Denver, CO
Ekshika Patel, BS1, Erin McArthur, MD, DPhil2, Garrett J. Weskamp, MD1, Bejan Saeedi, MD, PhD2, Robert T. Simril, MD3 1University of Colorado Anschutz Medical Campus, Denver, CO; 2University of Colorado, Denver, CO; 3Denver Health Medical Center, Denver, CO Introduction: Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have gained prominence for clinical benefits ranging from improved glycemic control and weight loss to cardiovascular risk reduction and renal protection. However, several landmark studies on GLP-1 RAs have also reported increased incidence of biliary disease, including increased rates of cholelithiasis and cholecystitis. Here, we present a case of severe acalculous cholecystitis resulting in Mirizzi-like syndrome after GLP-1 RA dose escalation.
Case Description/
Methods: A 63-year-old male with obesity, atrial fibrillation, hypertension, hyperlipidemia, GERD, and sleeve gastrectomy presented to the emergency room with one day of nausea, abdominal pain, and diaphoresis.
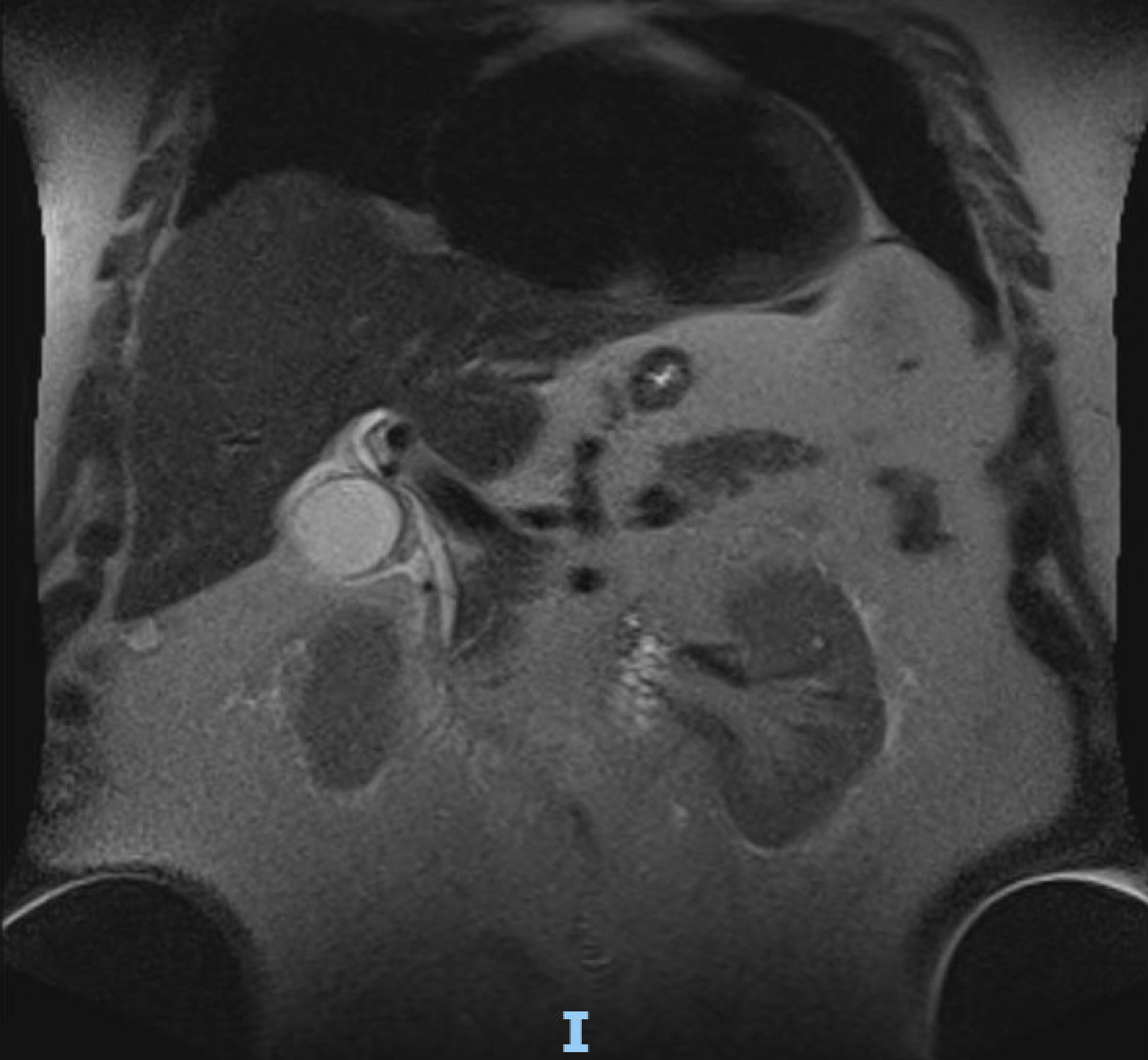
Initial vitals revealed a temperature of 36.2C, heart rate 108, respiratory rate 22, and his exam was notable for tenderness to palpation in the epigastrium. Labs indicated an acute liver injury with total bilirubin 9.0/direct bilirubin 5.1, AST 1831 U/L, ALT 1812 U/L, ALK 160 U/L, lactate 4.9, and lipase 47. Viral hepatitis labs, urine drug screen, acetaminophen and ethanol levels were all unremarkable. CT abdomen/pelvis showed hydropic gallbladder with wall thickening and fat stranding without hepatobiliary ductal dilation. Subsequent MRCP demonstrated compression of the common hepatic duct due to distension of the gallbladder up to 4.5cm in diameter. Blood cultures were positive for Klebsiella oxytoca. The patient underwent a laparoscopic cholecystectomy the next day revealing gangrenous cholecystitis without stones or obstruction noted on intraoperative cholangiogram. On day 1 post-op, his symptoms resolved, LFTs improved, and he was discharged home on a 7-day course of levofloxacin and metronidazole.
Notably, the patient stated he had lost 16 pounds since starting tirzepatide 3 months prior, and his dose was increased from 2.5 mg to 5 mg one week before presentation. Discussion: Common hepatic duct compression from acalculous cholecystitis described as a “Mirizzi-like” or acalculous Mirizzi syndrome after GLP-1 RA dose increase is a novel finding and could be related to inhibition of CCK by GLP-1. This case highlights the increased risk of biliary pathology with GLP-1 RA use, particularly during dose escalations. We recommend that providers consider the risk association between GLP-1 RA use and hepatobiliary pathology before prescribing and educate patients about possible biliary complications of GLP-1 RA use.
Figure: MRI/MRCP Pancreas showing compression of the common hepatic duct due to the distended gallbladder.
Disclosures: Ekshika Patel indicated no relevant financial relationships. Erin McArthur indicated no relevant financial relationships. Garrett Weskamp indicated no relevant financial relationships. Bejan Saeedi indicated no relevant financial relationships. Robert Simril indicated no relevant financial relationships.
Ekshika Patel, BS1, Erin McArthur, MD, DPhil2, Garrett J. Weskamp, MD1, Bejan Saeedi, MD, PhD2, Robert T. Simril, MD3. P0241 - A Rare Case of Mirizzi-like Syndrome in a Gastric Sleeve Patient With Recent GLP-1 RA Dosage Increase, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")