MedStar Georgetown University Hospital Washington, DC
Award: ACG Presidential Poster Award
Adam Khalaf, MD, Alessandra Martorella, DO, Alessandro El-Khoury, MD, Ade Waterman, MBChB, Walid Chalhoub, MD MedStar Georgetown University Hospital, Washington, DC Introduction: Homozygous methylenetetrahydrofolate reductase (MTHFR) mutations disrupt homocysteine metabolism and are associated with venous and arterial thrombosis. These patients may develop portal vein thrombosis (PVT) even in the absence of elevated homocysteine levels. Chronic PVT often leads to portal hypertension (PH), with variceal bleeding as the initial presentation in up to 15% of non-cirrhotic cases. In such scenarios, a transjugular intrahepatic portosystemic shunt (TIPS) may be indicated to reduce portal pressure. Typical complications post-TIPS include encephalopathy, shunt stenosis, or migration. We present a case of a patient with homozygous MTHFR mutation and non-cirrhotic PH who underwent TIPS placement and experienced recurrent sepsis episodes of unclear origin until endoscopic retrograde cholangiopancreatography (ERCP) confirmed a rare TIPS-common bile duct (CBD) fistula.
Case Description/
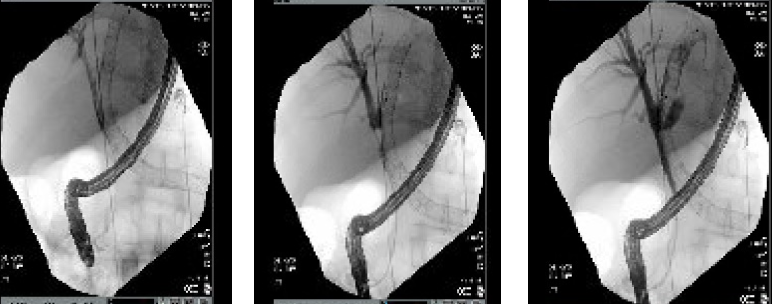
Methods: A 29-year-old man with MTHFR mutation presented with hematemesis and was found to have grade 3 esophageal varices, splenomegaly, and portal gastropathy, without cirrhosis. TIPS was placed despite portal-splenic vein thrombosis and required revisions for recanalization. This was complicated by recurrent episodes of sepsis of unknown origin. PET imaging revealed hypermetabolic activity within the intrahepatic TIPS, suggestive of endotipsitis. During an ERCP indicated for candidemia, guidewire advancement into the right intrahepatic ducts unexpectedly entered the TIPS lumen; occlusion cholangiography confirmed a TIPS–CBD fistula (Figure 1). Due to his complex vascular anatomy and thrombosed portal system, he was being evaluated for a combined liver and multivisceral transplant. Unfortunately, he developed secondary cirrhosis and complications related to extensive thrombosis, ultimately succumbing to septic shock at the age of 35. Discussion: A TIPS-CBD fistula is a rare and lethal complication, with only a few cases documented in the literature. In this case, while no single organism was consistently isolated across blood cultures, the infections mirrored published patterns, including gram-negative, fungal, and polymicrobial pathogens. This stems from biliary flora entering the systemic circulation via the fistula, consistent with endotipsitis. TIPS thrombosis is a strong risk factor for endotipsitis, and in patients with thrombophilic predispositions such as MTHFR mutation, the decision to pursue TIPS should be reconsidered. ERCP remains the gold standard for confirming a biliary fistula.
Figure: Figure 1: Sequential Fluoroscopic images from ERCP with occlusion cholangiography demonstrating extravasation of contrast from the biliary tree into the TIPS stent, consistent with a fistulous connection.
Disclosures: Adam Khalaf indicated no relevant financial relationships. Alessandra Martorella indicated no relevant financial relationships. Alessandro El-Khoury indicated no relevant financial relationships. Ade Waterman indicated no relevant financial relationships. Walid Chalhoub indicated no relevant financial relationships.
Adam Khalaf, MD, Alessandra Martorella, DO, Alessandro El-Khoury, MD, Ade Waterman, MBChB, Walid Chalhoub, MD. P0190 - Unexplained Sepsis After TIPS: A Rare Case of TIPS–CBD Fistula Diagnosed by ERCP, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



 photo")