Hally Chaffin, MD1, Caitlin Slaughter, PA-C1, Terry L.. Jue, MD2, Suryakanth Gurudu, MD1, Cuong Nguyen, MD1, Jeanne Palmer, MD1, Katalin Kelemen, MD, PhD1 1Mayo Clinic, Scottsdale, AZ; 2Mayo Clinic Arizona, Scottsdale, AZ Introduction: Myeloid sarcoma, also known as granulocytic sarcoma or chloroma, is an extramedullary tumor made up of immature myeloid cells, typically in the context of acute myeloid leukemia (AML). Extramedullary AML can present a diagnostic dilemma for clinicians, especially in the setting of uncommon organ involvement. Here we discuss a rare case of myeloid sarcoma presenting with pancreatic head mass and obstructive jaundice.
Case Description/
Methods: A 72-year-old man presented with 4 months of vague epigastric abdominal pain and CT abdomen/pelvis with findings of ill-defined, low-density mass concerning for pancreatic malignancy. CBC and hepatic function panel at that time were within normal limits. He underwent EUS which showed abrupt cut off of the main pancreatic duct at the pancreatic head and genu with subtle appearing 19 mm x 15 mm mass at the area. Fine needle biopsies were performed which resulted as chronic pancreatitis. Repeat imaging one month later reaffirmed presence of enlarging pancreatic mass and another EUS was performed. This showed 19 mm x 25 mm irregular mass in the genu of the pancreas. Biopsies were again consistent with chronic pancreatitis. Three months later he presented to the ED with obstructive jaundice (bilirubin 5.4), elevated AST, ALT, and alkaline phosphatase and leukopenia with severe neutropenia (ANC 240). Peripheral smear showed many circulating blasts. CT showed further enlargement of previously seen pancreatic mass with new intra and extrahepatic biliary ductal dilatation. He underwent ERCP and EUS which showed malignant-appearing biliary stricture which was treated with sphincterotomy and covered metal stent placement. EUS identified a mass in the pancreatic head, T2 N1 by endosonographic criteria. Fine needle biopsy was performed of the mass and an adjacent lymph node. Both samples were consistent with AML. He underwent bone marrow biopsy which was also consistent with AML and chemotherapy was initiated. Discussion: Incidence of extramedullary disease (EMD) in AML may be as high as 25-30%, typically occurring in the lymph nodes, spleen, and liver. Although EMD is common, pancreatic involvement of AML is exceedingly rare with only a few case reports in the literature. Many of these cases describe diagnosis of AML after surgical intervention. Bone marrow involvement of AML, such as in this case, may be present. It is important for clinicians to consider myeloid sarcoma when presented with these scenarios, particularly in the setting of vague workup.
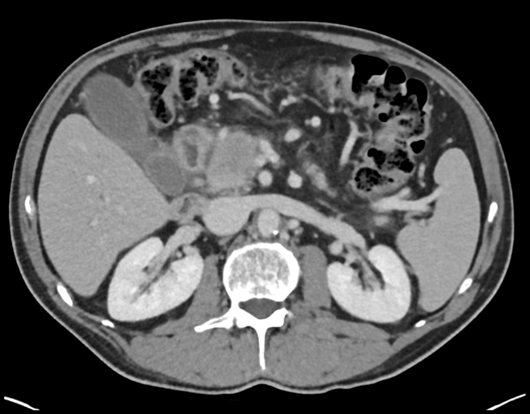
Figure: November 2024- subcentimeter pancreatic head mass present
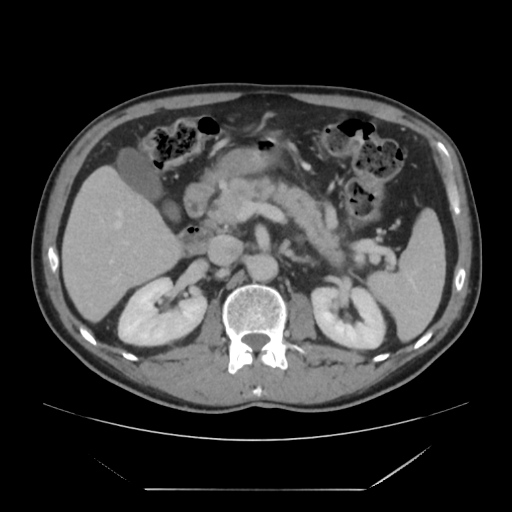
Figure: March 2025- enlargement of pancreatic head mass now measuring 2.9 x 2.6 cm
Disclosures: Hally Chaffin indicated no relevant financial relationships. Caitlin Slaughter indicated no relevant financial relationships. Terry Jue: Boston Scientific – Jan 2024, Honorarium received for serving as an Instructor at Fellows' Tissue resection course. Suryakanth Gurudu indicated no relevant financial relationships. Cuong Nguyen indicated no relevant financial relationships. Jeanne Palmer indicated no relevant financial relationships. Katalin Kelemen indicated no relevant financial relationships.
Hally Chaffin, MD1, Caitlin Slaughter, PA-C1, Terry L.. Jue, MD2, Suryakanth Gurudu, MD1, Cuong Nguyen, MD1, Jeanne Palmer, MD1, Katalin Kelemen, MD, PhD1. P0157 - Think Outside the Marrow: A Rare Case of Acute Myeloid Leukemia Presenting With Pancreatic Head Mass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")