Geisinger Wyoming Valley Medical Center Wilkes-Barre, PA
John K. Appiah, MD1, Danial Nadeem, MD1, Nikita Garg, MD1, Shivam Patel, MD1, Shaobo Zhu, MD2, Cherukuri Sreehari, MD1 1Geisinger Wyoming Valley Medical Center, Wilkes-Barre, PA; 2Geisinger Medical Center, Danville, PA Introduction: Perihilar cholangiocarcinoma (pCCA), or Klatskin tumor, is a rare malignancy arising at the hepatic duct confluence. It typically affects older adults with risk factors such as primary sclerosing cholangitis. Symptoms are often nonspecific, contributing to delayed diagnosis. We present a rare case of aggressive, widely metastatic pCCA in a previously healthy 37-year-old man.
Case Description/
Methods: A 37-year-old man presented with two weeks of painless jaundice, dark urine, and acholic stools. He reported a prior two-month history of cough, dyspnea, and fatigue, initially treated as pneumonia with doxycycline and prednisone. Jaundice developed shortly thereafter, raising concern for drug-induced liver injury. He later self-administered over-the-counter “liver detox” supplements. Exam revealed jaundice and hepatomegaly. Labs showed total bilirubin 15.0 mg/dL, ALT 361 U/L, ALP 796 U/L, and CA 19-9 >10,000 U/mL. Hepatitis serologies were negative. Imaging revealed a 4.5 cm left hepatic mass with intrahepatic biliary ductal dilation and suspicious pulmonary and osseous lesions. Endoscopic retrograde cholangiopancreatography (ERCP) showed a hilar stricture with poor left ductal filling. Endoscopic ultrasound-guided biopsy confirmed pCCA. Immunostaining was positive for CK7, CK19, and MOC31. Molecular profiling revealed a KRAS G12V mutation and CDKN2A loss. PD-L1 expression was < 1%, and tumor mutational burden was low. Despite supportive measures, the patient rapidly declined and later passed due to respiratory failure. Discussion: This case illustrates an atypically aggressive presentation of pCCA in a young adult without known risk factors. Metastatic spread to the lungs and bones is rare at initial diagnosis, and respiratory failure is an uncommon terminal event. Early imaging and specialist referral are essential when evaluating cholestatic liver enzyme elevations in patients with systemic symptoms, regardless of age. This case highlights the need for vigilance in the differential diagnosis of painless jaundice, even in young adults.
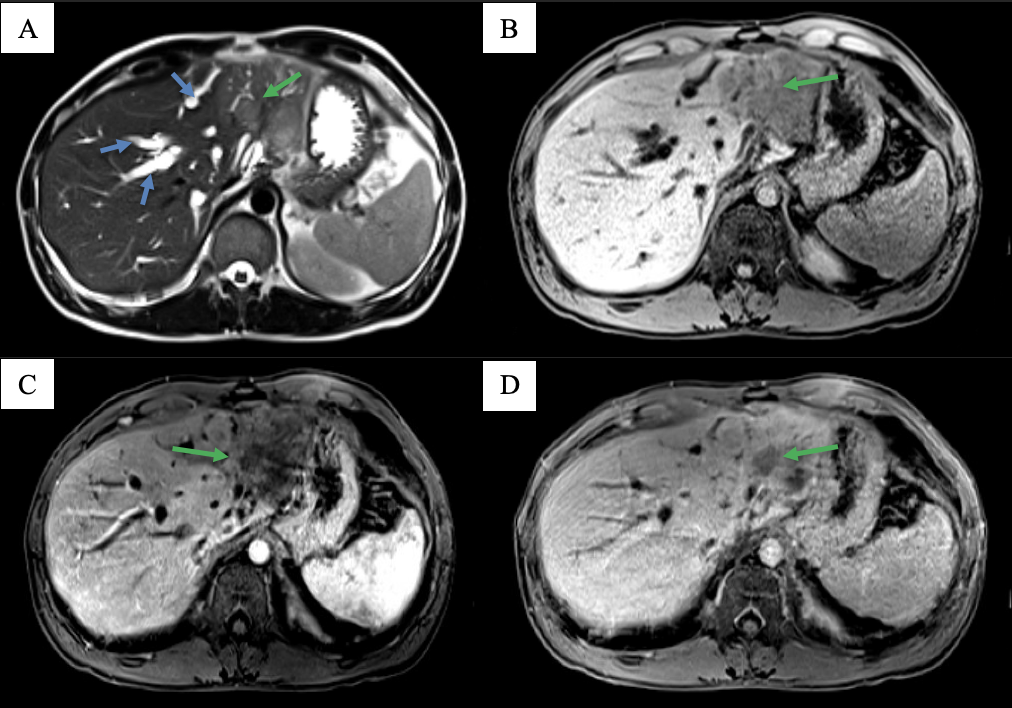
Figure: Figure 1: MRI axial T2 (A), T1 fat saturated pre-contrast (B) and early (C) and delayed (D) post-contrast sequences. A large mass (green arrow) in the left hepatic lobe demonstrates mild T2 hyperintense signal and causes intrahepatic ductal dilatation (blue arrows). The mass has T1 hypointense signal (B) and shows early peripheral (C) and subsequent progressive enhancement (D), characteristic of cholangiocarcinoma.
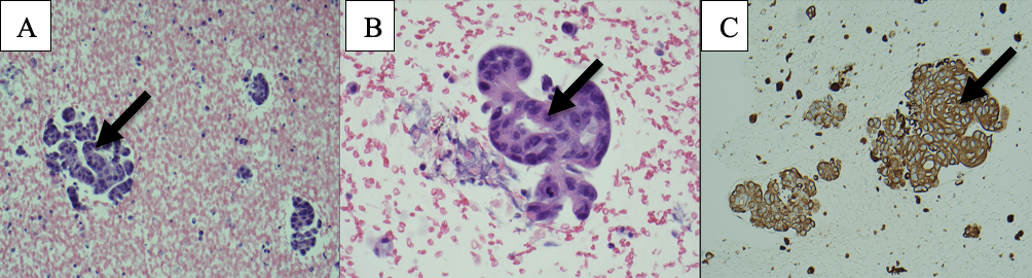
Figure: Figure 2 Histological slides of cholangiocarcinoma A: Low power (10X H&E) view of the cellblock of liver biopsy shows groups of malignant epithelial cells with glandular formation. B: High power (40X H&E) view of the cellblock of liver biopsy shows the malignant epithelial cells with pleomorphic vesicular nuclei and prominent nucleoli. C: High power (40X) view of the immunohistochemical stain for CK7 with diffuse strong cytoplasmic staining.
Disclosures: John Appiah indicated no relevant financial relationships. Danial Nadeem indicated no relevant financial relationships. Nikita Garg indicated no relevant financial relationships. Shivam Patel indicated no relevant financial relationships. Shaobo Zhu indicated no relevant financial relationships. Cherukuri Sreehari indicated no relevant financial relationships.
John K. Appiah, MD1, Danial Nadeem, MD1, Nikita Garg, MD1, Shivam Patel, MD1, Shaobo Zhu, MD2, Cherukuri Sreehari, MD1. P0144 - Caught Yellow-Handed: An Unusual Case of a Klatskin Tumor in a Young Adult, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.